Academic Paper Series
2012
Contents:
Foreign and Domestic Economies of North and South Korea The Markets of Pyongyang Similar Policies, Di erent Outcomes: Two Decades of Economic Reforms in North Korea and Cuba KORUS FTA Compared with KOREA-EU FTA: Why The Di erences? Developing an International Financial Center to Modernize the Korean Service Sector Security Factors and Regional Impact on the Korean Peninsula Preparing for Change in North Korea: Shifting Out of Neutral Reviving the Korean Armistice: Building Future Peace on Historical Precedents Proactive Deterrence: The Challenge of Escalation Control on the Korean Peninsula Human and Nuclear Security Concerns on the Korean Peninsula Engaging North Korea on Mutual Interests in Tuberculosis Control 2012 Nuclear Security Summit: The Korean Twist
Volume 5
Korea Economic Institute
ON KOREA 2012: ACADEMIC PAPER SERIES Volume 5
Human and Nuclear Security Concerns on the Korean Peninsula
Engaging North Korea on Mutual Interests in Tuberculosis Control
Sharon Perry, Heidi Linton, Louise Gresham, and Gary Schoolnik Sharon Perry served as director of the Stanford DPRK TB Laboratory Project from 2008 to 2011, and is a member of the National Committee on North Korea. Heidi Linton is executive director of Christian Friends of Korea, Black Mountain, North Carolina; Louise Gresham is director of the Global Health and Security Initiative, Nuclear Threat Initiative, Washington, D.C.; and Gary Schoolnik is associate dean and professor of medicine at Stanford University School of Medicine, Stanford, California. Relations on the Korean Peninsula are at their coolest level in more than 20 years. Since 2006, when the Democratic Peoples Republic of Korea (DPRK) announced that it had restarted its nuclear facilities, the government has challenged international nonproliferation treaties on several occasions. The death of Kim Jong-il in December 2011 as well as plans for transfer of leadership to his youngest son, Kim Jong-un, bring new complexities to government relations with the outside world. Following military incidents in 2010 along the long-disputed Northern Limit Line in the Yellow Sea, the North has reinforced its relations with China while pulling back on negotiations with the United States and its allies.1 The DPRK is a foreign policy conundrum. While the regimes nuclear ambitions remain at the forefront of international security concerns,2 the world is painfully aware that this isolated and enigmatic country of 24 million people is also plagued by crippling energy, food, and medical shortages.3 Since the famines of the 1990s, rates of tuberculosis (TB), a disease that exploits malnutrition and other conditions that compromise natural immunity, have risen dramatically and are now among the highest in the world outside of sub-Saharan Africa, including more than triple the rates in China and South Korea.4 From 1995 to 2003, the U.S. government provided more than a billion dollars in food, energy, and medical assistance to North Korea.5 Absent an impact of humanitarian efforts on broader diplomatic opportunities, international humanitarian contributions have fallen off dramatically in recent years even as the North Korean economy continues to struggle. In the decade since the breakdown of the Agreed Framework, it is increasingly apparent that policies tying economic aid to nuclear disarmament are not working.6
2012 Volume 5
ON KOREA
In this paper, we describe our experience working with the civilian DPRK Ministry of Public Health (MoPH) to develop the countrys first modern TB laboratory.7 Begun in 2008, this unique collaboration of U.S.-based voluntary interests, including a major medical institution, a humanitarian nongovernmental organization (NGO), and a nonprofit sponsor, has achieved cooperation on a critical public health objective during a period otherwise marked by profound deterioration of relations with the United States and its allies in East Asia. Because coordinated global efforts are needed to control TB in the antibiotic era, we argue such engagements can encourage broader assimilation within the international health community. We first provide background on the modern history of TB epidemics, the new challenges to global health security posed by the emergence of drug-resistant strains, and how these epidemics can interact with major geopolitical events. We hypothesize that the TB situation in North Korea today bears ominous parallels with conditions accompanying the end of the Cold War in Europe and that Northeast Asia faces a similar set of challenges as it contemplates opportunities for assimilation. We then describe the process of implementing the laboratory project and our objectives for sustaining this effort. We conclude by discussing implications of these efforts for North Korea and global health security interests.
Tuberculosis and Health
M. tuberculosis, the cause of human tuberculosis, is an airborne pathogen that chronically infects more than one-third of the worlds population, causing more than nine million cases of active TB and nearly three million deaths each year.8 Classically associated with conditions of poverty, malnutrition, aging, and medical conditions that suppress the immune system, 80 percent of cases occur in the developing world. Because of its intimate association with general health, particularly in adults of reproductive age, the World Bank and the World Health Organization (WHO) have characterized TB control as one of the most cost-effective investments developing countries can make.9 A pathogen of humans for more than 50,000 years,10 M. tuberculosis has developed strategies for interacting with the human life span. The natural history is characterized by three principal stages: exposure, latent infection, and active disease with transmission to new hosts ENREF 5.11 Of those exposed to an infectious TB case, about 30 percent are thought to develop the state of latent infection, during which the host remains
Perry, Linton, Gresham, and Schoolnik: Engaging North Korea
healthy, but TB bacilli may survive for decades within clusters of immune cells. Latent infections constitute the pathogens population reservoir. Although the normal human immune system is substantially equipped to control a latent infection, in 10 percent of these infections, the latent state is terminated by a breakdown in immune defenses brought on by malnutrition, illness, or aging, and the individual develops the active, contagious form of the disease. Without treatment, about 50 percent of active cases will die, and each infectious case at this stage will disseminate the TB bacillus to 10 to 20 other persons.12 In this way, M. tuberculosis is able to infect successive human generations. In the pre-antibiotic era, TB epidemics could rage for centuries, devastating isolated populations weakened by hunger and acute infections.13 Although antibiotics have greatly improved the treatment outcome for TB, current therapy still requires the combined use of at least four different antibiotics administered in an uninterrupted manner for at least six months.14 Because TB capitalizes on any condition that jeopardizes the individuals general health, attention to the patients nutritional status and underlying medical conditions is also required. The use of fewer drugs, interruption of drug therapy, inadequate nutrition or intervening illness can result in poor clinical outcome (including death) and the dissemination of TB to other persons. For these reasons, control of TB requires primary-care approaches and rational drug management strategies, including sustainable, stable, public health structures.
Drug-Resistant Tuberculosis
The discovery of curative drugs in the middle of the 20th century, including their application to massive global public health campaigns, came at a critical time in the political realignment of the postwar world and the emergence of modern global markets. These developments have fundamentally altered the course of TB epidemics, particularly in the West. For example, rates of TB in the United States today are 3.6 per 100,000 population (compared with a global average of 137 per 100,000 in 200915) compared with 53 per 100,000 in 1953 when the first anti-TB drugs were introduced.16 By the late 20th century, howeverwithin the short span of one human generationtwo developments began to threaten these gains. The first, during the 1980s, was the emergence of AIDS, a disease that attacks the
10
2012 Volume 5
ON KOREA
same immune cells required to control a latent TB infection. The AIDS epidemic has had a profound impact on TB trends, particularly in Africa where up to 30 percent of new TB cases may be due to HIV co-infection.17 The second development was the emergence of multidrug-resistant strains of TB (MDR TB), first reported in the early 1990s.18 MDR TBdefined as resistance to at least isoniazid and rifampicin, the two most powerful front-line TB drugsaccounted for nearly a half million cases of TB annually, including an estimated 150,000 deaths, in 2008.19 Treatment of MDR TB requires up to two years of complex drug management with regimens that often have toxic side effects and are 50200 times more costly than drugs needed to treat persons with TB caused by drug-sensitive strains.20 Although survival rates are improving, they are only marginally better than those of the pre-drug era. Cases of extensively drug resistant TB (XDR TB), defined by resistance to the major first- and second-line TB drugs and largely incurable, have now been reported in 58 countries with the laboratory capacity to test for it, and it may account for up to 10 percent of MDR TB cases globally.21 These trends raise the specter of an era in which current drugs are no longer effective. Resistance to TB drugs arises from spontaneous mutations in the TB genome under drug selection pressure, conditions that are associated with sporadic drug use, including poor patient adherence, as well as use of unregulated drug supplies. In this regard, drug-resistant TB is a preventable man-made phenomenon. Drug mutations develop rapidly in the setting of monotherapy (use of only one drug for treatment) and will amplify quickly to affect remaining drugs in the armamentarium.22 For this reason, compared with new TB patients, risk of MDR TB is about 5.5 times greater in patients who have received inadequate therapy in the past.23 Because MDR TB may develop over months or years, inadequately treated persons who continue to be infectious can spread drug-resistant strains to persons in their communities.24 If inadequately treated persons migrate across frontiers, drug-resistant strains can be spread to other populations. In absolute numbers, about 50 percent of MDR TB cases occur in China and India although the highest proportions of TB cases with MDR (9 percent of the worlds cases) reside in eastern Europe and Central Asia.25 As many as 50 percent of cases in countries of the former Soviet Union are resistant to at least one TB drug.26 In parts of the Russian Federation and the countries of Kazakhstan, Tajikistan, Uzbekistan, and the Republic of Moldova, 25 percent of new TB patients and more than 50 percent of
Perry, Linton, Gresham, and Schoolnik: Engaging North Korea
11
previously treated patients suffer from multidrug-resistant disease.27 The age of these victims peaks in young adulthood, suggesting a relatively recent introduction.28 Multidrug-resistant strains may have been amplified by prolonged drug shortages that occurred during the period of economic destabilization accompanying the collapse of the Soviet bloc in the 1980s.29 With the end of the Cold War in Europe, drug-resistant strains from this epicenter have now been tracked by molecular fingerprinting methods to North America, Europe, the Middle East, and even to South Africa.30 The magnitude and dissemination of the MDR epidemic in the Eurasian region and South Africa caught the world off guard and caused a reevaluation of global strategies for TB control. Laboratories with capacity to test for drug resistance were not available in most high-burden countries,31 and it was quickly recognized that the cost of treating MDR and XDR far exceeds public health budgets of developing countries.32 Since 2000, massive resources have been organized through the STOP TB Partnership (www. stoptb.org) to manage MDR and XDR TB and control its spread. A major driver in the MDR TB scale-up effort has been the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), which in 2011 contributed $700 million to global MDR TB control.33 Global Fund works closely with the Green Light Committee, which recommends standards for MDR TB care,34 and the Global Laboratory Initiative, which sets quality assurance standards for drug susceptibility testing and works to accelerate access to modern TB diagnostics.35 With additional support from programs like the Presidents Emergency Plan for AIDS Relief (PEPFAR), the Obama Global Health Initiative, UNITAID, and the Foundation for Innovative Diagnostics (FIND), 27 high-burden MDR TB countries15 of which were states of the former Soviet blochave been targeted for aggressive scale-up operations.36 The Soviet experience shows that drug-resistant strains of TB, generated in one region as a consequence of failed public health programs, can disseminate to spawn outbreaks of drug-resistant disease both regionally and remotely. This experience also reminds us that MDR epidemics leave costly legacies for which the world community is ultimately responsible. We contend that political and economic conditions coinciding with the emergence of new drug-resistant strains in the former Soviet Union still persist in Northeast Asia.
12
2012 Volume 5
ON KOREA
Tuberculosis in North Korea Health System
TB care in North Korea was heavily influenced by the Soviet model of centralized administration and sanatorium care. During the 1960s and 1970s when Soviet bloc subsidies were plentiful, North Korea implemented a universal health care program (Article 72 of the Constitution), and developed its household doctor system. At a reported coverage of 1 doctor per 134 households, this system boasts one of highest coverage ratios in Asia even today.37 During this period, the No. 3 (TB) Prevention Department of the MoPH built a multitiered residential treatment system for TB with its own pharmaceutical industry, including 10 provincial TB hospitals as well as a system of 6070 bed TB rest homes in each of the countrys approximately 225 counties and municipal districts.38 Since the loss of Soviet aid in the 1990s,39 much of the public health infrastructure, including physical plant and medical equipment, has not been updated, and the TB pharmaceutical industry has virtually disappeared. Although the health system remains largely intact organizationally, chronic energy, equipment, and supply shortages plague operations at every level. Today the country relies almost entirely on a dwindling supply of donors for basic medical supplies, including TB drugs and diagnostics. The DPRK is not eligible for basic health sector development funds, such as through the World Bank, International Monetary Fund, or the Asia Development Bank.
Epidemiologic Trends
In 1998, WHO established a country office in Pyongyang.40 This program, which is supported by continuing cooperative planning agreements between the WHO and the government, provides one source of documentation of health trends inside the DPRK. These and other planning documents make it clear that the famines of the mid-1990s had a profound impact on the general health status of the population, including rates of infant and maternal mortality, hepatitis, malaria, and TB.41 From 1996 to 1999, rates of mortality due to TB tripled to more than 100 per 100,000 population, rivaling some of the worst rates in the developing world.42 Average caloric intake in DPRK has steadily declined over the past 20 years and is the lowest in the Asia-Pacific region; North Koreas current caloric intake per person is less than two-thirds of that of China and the ROK.43 The Organization for Economic Development (OECD) estimated that 32 percent of the population was malnourished in 2006,
Perry, Linton, Gresham, and Schoolnik: Engaging North Korea
13
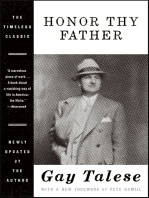
and a survey jointly sponsored in 2009 by the World Food Program, Food and Agriculture Organization, and UNICEF estimated that 32 percent of children are of stunted height, 18 percent underweight, and 5 percent of low weight for height.44 A new United Nations census released in 2010 estimates that life expectancy has declined by 3.4 years (to 69.3 years) since 1993, while infant and maternal mortality rates, each among the highest in the Asia-Pacific region, have risen 36 percent and 46 percent, respectively, in the same period.45 TB caseload estimates provided to WHO by the MoPH for 1994, the period just before the great famines, show a TB incidence rate of about 38 per 100,000 population.46 Although these figures pre-date the development of standardized reporting systems, such rates are similar to those reported in other Soviet-style systems of the era and would be in a range reported by middle-income countries today. In 2001, MoPH adopted the WHOsponsored Directly Observed Short Course Therapy (DOTS) program for TB control, including its treatment standards and reporting formats.47 In 2006, three years after this program was implemented nationwide, an incidence rate of 178 per 100,000 was reported.48 In 2009, following a small community infection survey,49 WHO doubled its estimates of TB incidence to 345 per 100,000 population.50 For 2010, North Korea is expected to require drugs for nearly 100,000 TB patients, translating to a case rate more than 370 per 100,000 population.51 Compared with the 22 historically designated highburden countries,52 TB incidence in North Korea ranks number seven or number eight in the world, being one of the highest outside of sub-Saharan Africa and nearly four times the rates in China (78 per 100,000) and South Korea (97 per 100,000) in 2010 (Figure 1).53 These trends are not due to poor program performance, as DPRK maintains very high case detection and treatment completion rates within the WHO DOTS program.54
14
2012 Volume 5
ON KOREA
Figure 1: Trends in Incidence of Tuberculosis in East Asia, 19902010
450 400 350 300 250 200 150 100 50 0 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010 DPRK ROK China Mongolia
Source: WHO, Global Tuberculosis Control 2011 (Geneva: World Health Organization, 2011), Annex 3.Age-specific case trends and an annual risk of TB infection estimated at 3.2 percent suggest the epidemic is still expanding (at perhaps 10 percent per year),55 plausibly fanned by continuing food shortages and acute infections such as measles that are known to suppress the immune system.56
TB Assistance to North Korea
As a low-income country (less than $1,000 annual income per capita) with a TB incidence rate in excess of 100 per 100,000, the DPRK meets highpriority conditions for assistance through the world STOP TB partnership of funds. From 2001 through 2007, the country received basic TB drugs and diagnostic supplies through the WHO-sponsored Global Drug Facility (GDF). However, the adequacy and sustainability of this assistance, often supplemented by NGO donations,57 have been complicated by the countrys diplomatic isolation. In 2003 and 2006, for example, the country lost bids to qualify for longer-term TB assistance through the Global Fund. Following the nuclear test in 2006, a $400,000 grant from the Canadian International Development Agency (CIDA) to WHO for expansion of TB programs in the DPRK was withdrawn.58 In 2010, following two exceptional years of bridge funding through GDF and WHO regional budgets, the Global Fund reached an agreement with the DPRK that is expected to continue first-line TB medicines for at least another two years and also enable planning for MDR TB surveys and treatment programs. Because the DPRK is subject to the Global Funds additional safeguards policies, UNICEF has been appointed
Perry, Linton, Gresham, and Schoolnik: Engaging North Korea
15
principal recipient for the countrys TB and malaria grants.59 Because of recent shortfalls in Global Fund accounts, funds for the continuation phase of this grant are likely to be subject to significant cuts.60 As a result of this problematic funding history, critical capacity needs of the DPRK national TB program have been postponed even as the countrys epidemic has continued to expand. The precise magnitude of this epidemic is uncertain, however, because published epidemiologic data may differ from statistics heard by NGOs on the ground, and Web resources often present differing estimates. In addition to basic energy and nutritional needs not covered by standard TB program assistance, one of the most critical of the postponed agendas has been development of resources to diagnose and treat drug resistance. Until initiation of the U.S.-DPRK Tuberculosis Project, the DPRK national TB program was one of the few operating in a country with a TB incidence rate over 300 per 100,000 population that lacked funding for development of at least one facility for diagnosis of TB by culture and drug susceptibility testing. In the absence of such facilities, the contribution of drug resistance to this epidemic, including the types of drugs needed to treat patients who fail to respond to standard therapy, cannot be determined. Although the DPRK is not a candidate for the global MDR scale-up effort targeted to high-burden countries, rates of drug resistance are likely to be significant, a prediction based on retreatment rates reported to WHO as well as regional trends.61
Regional Implications
The DPRKs TB epidemic has important implications for Northeast Asia, including provinces of northeast China, Mongolia, and neighboring oblasts of the Russian Federation. Rates of drug resistance in Northeast Asia are some of the highest in the world outside of the Russian Federation, with which the area shares extensive borders. In 2008, the China Center for Disease Control reported that rates of drug resistance in the northeastern provinces of Inner Mongolia Autonomous Region, Liaoning, and Heilongjiang exceeded 7 percent among new cases of TB and ranged from 24 percent to 37 percent among previously treated cases. A small nationwide survey carried out in Mongolia during 1999 found rates of isoniazid mono-resistance to be as high as 30 percent, although rates of multidrug resistance may be lower than in neighboring areas owing to the relatively late introduction of rifampicin in that country.63 High background rates of MDR TB, especially among previously treated patients in this region, may be due to shared historical circumstances. Public health systems in this part of the world are still recovering economically
16
2012 Volume 5
ON KOREA
from the breakup of the communist bloc. Older, sanatorium-style systems of TB care are common, and much of the laboratory infrastructure requires upgrading.64 Many countries in the region have experienced unprecedented prosperity and are just beginning to launch MDR scale-up programs. Although more than one-half of the worlds MDR burden occurs in China, India, and other parts of East and Southeast Asia,65 less than 4 percent of these cases have been been enrolled in treatment programs to date.66 Compared with 12 in the European region,67 there are only three certified supranational TB reference laboratories (in Chennai, Bangkok, and Hong Kong) serving the entirety of continental Asia. South Koreas supranational TB reference laboratory, a designated training center in the international reference and research system, is inaccessible to North Korea. In short, because of the constraints of Cold War relations, this region is poorly prepared to respond to a collapse of TB care on or within its borders. For this reason, the response to the DPRK TB epidemic must also be looked at in the context of supporting an important health security agenda for an epidemiologically vulnerable region of the world. In summary, the TB epidemic in the DPRK has evolved ominously since the breakup of the Soviet Union and the famines of the 1990s. In contrast with the Soviet experience, and in part in response to it, the global health community is far better organized today to ensure that no country, regardless of its political system, goes without basic TB drugs. At the same time, because of continuing diplomatic isolation, the country remains off the radar for internationally funded MDR scale-up programs. This should be seen as an urgent regional priority.
The U.S.-DPRK Tuberculosis Project Goals
The goals of the U.S.-DPRK Tuberculosis Project are to develop sustainable professional and academic collaborations with the North Korean Ministry of Public Health focused on mutual interests in TB control and to facilitate networking with other TB programs in the region and internationally.
History
The concept for this project arose indirectly from unofficial discussions attending the so-called track 2 arm of the six-party talks. In February of 2007, during the fifth round of the six-party talks, the DPRK agreed to phase out the Yongbyon nuclear plant in exchange for economic assistance and eventual normalization of relations.68 Working with this framework, Stanford professor of political science, John W. Lewis, solicited School
Perry, Linton, Gresham, and Schoolnik: Engaging North Korea
17
of Medicine colleagues to assess the prospects of engagement focused on mutual interests in TB control. Following these discussions, Lewis obtained approvals for a delegation of DPRK public health officials to meet with TB specialists at Stanford. In January 2008, with sponsorship from the Freeman-Spogli Institutes Center for International Security and Cooperation (CISAC) and Walter H. Shorenstein Asia-Pacific Research Center (APARC), four DPRK MoPH officials and one protocol officer spent a week in northern California, touring TB facilities in the San Francisco Bay Area (Figure 2). The Bay Area TB Consortium (Stanford/BATC), an affiliation of TB physicians, microbiologists, and epidemiologists drawn from the areas medical schools and public health departments, was organized by Stanford School of Medicine to host the delegation along with ex officio representatives from the Korea Society, Eli Lilly Foundation, the U.S. Centers for Disease Control and Prevention (CDC), and WHO. Figure 2: MoPH Delegation at Stanford University, 12 January 2008 During these discussions, MoPH representatives, led by the director general of the No. 2 and No. 3 (TB and Hepatitis) Departments, requested assistance to complete a modern TB reference laboratory at the campus of the No. 3 (TB) Prevention Hospital in the capital city of Pyongyang. Although WHO and MoPH had devised a site plan and equipment inventory for this project in 2006, the initiative had since stalled for lack of funds.69
Implementation
From this seminal meeting at Stanford, the U.S.-DPRK Tuberculosis Project evolved into the partnership of the Stanford Bay Area TB Consortium, the Nuclear Threat Initiative/Global Health and Security Initiative (NTI/Global Health and Security Initiative), and Christian Friends of Korea. Since 2009, these organizations have contributed a combined total of more than $600,000 and have completed more than 12 in-country visits to develop the DPRKs first modern TB laboratory. Despite significant diplomatic reversals coinciding with our schedule, momentum was not affected, and U.S. teams
18
2012 Volume 5
ON KOREA
experienced extraordinary cooperation from MoPH and other government officials. Implementation of the project has progressed through four principal stages, including organizational development, site assessments, installations, and technical training (Figure 3). Figure 3: U.S.-DPRK Tuberculosis Project Implementation Schedule
Choenan Incident
U.S. food program ends 2010-Present BATC Training 2010 Workshops Dedica on Ceremony 2009 Deliveries & Installa ons 2008 CFK on-site visit 2008 MOPH visit to Stanford Yeongpyong Island Incident
Missile Test, Nuclear Test
Source: Authors concept.
Organizational development (March 2008December 2008).
Shortly after the meeting at Stanford, organizers obtained the proposed TB laboratory inventory from WHO representatives in Pyongyang and, with assistance of Dr. Gail Cassell of the Eli Lilly Foundation, successfully applied to the NTI/Global Health and Security Initiative of the Nuclear Threat Initiative for funds to carry out site assessments and purchase the recommended equipment and supplies. During this phase, Stanford organizers also initiated contacts with the U.S.-DPRK NGO community and established ongoing working relations with world health officials in Pyongyang, New Delhi, and Geneva to ensure that laboratory donations conformed to international standards and plans for the DPRK. In October 2008, Christian Friends of Korea (CFK), a U.S. NGO with more than 15 years of experience provisioning and renovating TB facilities in North and South Hwanghae provinces, was able to visit the proposed laboratory site during one of its regular in-country technical missions. CFK developed a physical infrastructure report, identifying an additional budget for infrastructure renovations, including plumbing and electrification, needed to support the proposed Stanford and NTI equipment donations.
Perry, Linton, Gresham, and Schoolnik: Engaging North Korea
19
On the basis of these assessments, in December 2008, Stanford and CFK approached the DPRKs mission to the United Nations in New York to propose a joint undertaking. Under this plan, CFK agreed to organize logistics and in-country visits, secure necessary U.S. export licenses, and complete physical renovations in cooperation with MoPH and local hospital staff. Stanford/BATC agreed to assess TB laboratory technology needs, procure the TB laboratory inventory in collaboration with its funding sponsor, and organize in-country expert training workshops. Thus, the project built upon a previously established foundation in U.S.DPRK NGO relations and evolved to combine a strong mix of U.S.-based scientific, humanitarian, and health policy expertise in TB control.
On-site assessments (April 2009September 2009).
Following MoPH acceptance of this proposal, joint Stanford/CFK site assessment teams visited the laboratory site in May and August of 2009 (Figure 4) to develop work plans and procurement specifications in consultation with MoPH and WHO representatives. Technical expertise on the assessment teams included a construction engineer, a biomedical engineer, and a clinical laboratory consultant from CFK and, on behalf of the Stanford/BATC, a supervising scientist from a TB public health laboratory in California and a TB epidemiologist from Stanford School of Medicine. Three coordinators from the MoPHs Department of External Affairs were assigned to facilitate in-country delegations during the first on-site assessment visit, and they have remained invaluable partners of the project ever since. Figure 4: Site Planning Visit, May 2009 Based on these site assessments, license applications for renovation materials and laboratory supplies were submitted to the Bureau of Industry and Security of the U.S. Department of Commerce. Following approvals in the summer of 2009, procurements were completed and prepared for shipment during September 2009.
20
2012 Volume 5
ON KOREA
Delivery and installation (November 2009October 2010).
From 29 October to 24 November 2009, a 22-member revolving delegation, including CFK and Stanford/BATC work teams and a representative from the NTI/Global Health and Security Initiative, spent nearly a month working at the laboratory site in Pyongyang. Scores of MoPH personnel (including lab staff, doctors, nursing students, and volunteers) worked side by side with skilled CFK volunteer construction teams to remodel rooms, install electrical and plumbing systems, and build workbench spaces (Figure 5). A CFK bioengineer together with a team of Stanford/BATC laboratory trainers and MoPH laboratory physicians installed and tested several pieces of equipment. Two additional visits in May and August of 2010 were required to complete the renovations and verify inventory. During the summer of 2010, CFK raised additional funds and oversaw the installation of a four-kilometer dedicated high voltage cable connecting the laboratory to the municipal power supply. Figure 5: CFK and MoPH Work Crews Threading New Electrical Lines, November 2009 With physical plant installations completed, DPRKs first TB laboratory designed to perform reference-level quality assurance, culture, and drug-susceptibility testing was formally dedicated on 18 October 2010 in a ceremony hosted by the vice minister of the Ministry of Public Health. In addition to representatives from Stanford/ BATC and CFK, officials from the WHO Pyongyang office, UNICEF (the new Global Fund agent for the DPRK), and staff from the No. 3 (TB) hospital campus were in attendance.
Training and technical assistance programs (November 2010present).
The Stanford/BATC team includes public health laboratory specialists from the state of Californias TB laboratory system, the Stanford Hospitals Clinical Microbiology Laboratory, and infectious disease faculty from the Stanford School of Medicine, as well as outside consultants. Individual members of this group have extensive experience in international health, including service on WHO and CDC working committees, and on advisory panels of country-based infectious disease control programs.
Perry, Linton, Gresham, and Schoolnik: Engaging North Korea
21
Figure 6: National Tuberculosis Reference Laboratory, Joint BayArea TB Consortium-MoPH Training Workshop, October 2010 This team is complemented by CFK professional volunteers, including a clinical laboratory professor, a bioengineer with extensive experience in international settings, and a retired clinical microbiologist fluent in Korean. Since November 2009, these teams, in collaboration with MoPH physicians and laboratory technicians, have been conducting orientation and training workshops covering basic safety procedures, inventory maintenance, and standard operating procedures for culture and drug susceptibility testing (Figure 6). The project also seeks to foster regional affiliations for TB control and in April 2011 sponsored a visit by seven MoPH officials to the Shanghai Centers for Disease Control. Additional workshops and training exchanges are planned through 2012.
Future of the Project
Located within the No. 3 (TB) Prevention Hospital, DPRKs new national TB reference laboratory is a 2,500-square-foot facility, including 13 rooms modeled and equipped to international laboratory standards and a dedicated power supply to run incubators and other essential equipment on a 24-hour basis. The laboratory has a staff of 15 administrators, physicians, and technicians. Three laboratory physicians have been with the project since the meeting at Stanford in 2008. The laboratory project has also served as a catalyst for additional investments in central TB control. With the help of CFK, the Central TB Preventive Institute in Pyongyang, where the laboratory is housed, has since completed a stateof-the-art operating room suite and installed three greenhouses for food production, with additional plans in 2012 to develop classroom facilities.
Role of the laboratory in tuberculosis control.
To prepare for its role in national TB control, the new reference laboratory must undergo international inspections and participate in field trials designed to assure the reliability and quality of laboratory results. Ultimately, the plan is to develop capacity to test several thousand
22
2012 Volume 5
ON KOREA
cases of suspected MDR TB per year. The laboratory is also expected to develop capacity to provide surveillance for the national TB control program, determine prevalence of drug resistance in North Korea,70 and guide treatment in patients suspected of having drug resistance.71 By offering modern, reference-level diagnostic and clinical consultation services, the laboratory can also serve as a national resource or center of TB excellence for physicians, laboratorians, and medical and laboratory trainees throughout the country. This resource can also help integrate TB care provided by other ministries into the MoPH DOTS program. We believe these goals are feasible over the next two to three years, particularly if MoPH is able to build academic collaborations with scientific teams such as the BATC and develop affiliations with international laboratory and medical organizations. The high literacy rate in the DPRK and the competencies observed by the BATC training team also suggest that MoPH possesses the human capital needed to realize these goals. The project is currently working with the WHO country office to assess continuing training needs in order to strengthen qualifications for international accreditation and create opportunities for collaborative research on MDR TB with academic institutions in the region as well as abroad.
Factors contributing to success.
The momentum of this project has depended on several interrelated factors. First, from a political perspective, the project benefited from the initiative of policy specialists at the outset to recognize an opportunity for health engagement during a period when work toward normalization of relations with the United States seemed possible. Second, the project addresses a public health priority (TB control) that is recognized at the highest levels of the DPRK government. The expertise assembled through the Bay Area TB Consortium and efforts to involve world health authorities in planning are important as MoPH moves toward qualifications for broader international support. Third, NTI/Global Health and Securitys prior work building cooperation across disputed borders and recognition of the need for cooperative disease surveillance72 led to critical funding support for laboratory donations. Having this funding secured at an early stage of planning helped greatly to spur the organizational partnerships needed to implement the project. Fourth, the preexistence of a highly valued NGO relationship with CFK, including CFKs reputation for trust building, follow-through, and sincere humanitarian focus, was a critical factor in gaining acceptance from government officials on both sides of the Pacific. Fifth, academic institutions must be prepared to anticipate
Perry, Linton, Gresham, and Schoolnik: Engaging North Korea
23
significant infrastructure needs in the DPRK that are precedent to building productive program collaborations. Thus, partnering with CFK also brought important experience and capacity to address critical renovation and electrical power needs associated with TB programs in the DPRK. Finally, the continuity of personnel on both sides enabled an atmosphere of mutual understanding and focused persistence to flourish. Many challenges along the waysuch as delivery delays, freezing temperatures, retrofitting problems, sickness on the work teams, and the need to improvise training conditions in the early stagescould have derailed the initiative. These were overcome cheerfully and in good faith and have contributed to strengthening ties between the U.S. and DPRK teams. At the same time, the next stage of this projectto support accreditation of the laboratory through training partnerships and operational research collaborationis critical to establishing the sustainability of our efforts and the potential for this unique U.S.-DPRK cooperation to have a meaningful impact on TB trends in the DPRK.
Implications
The modern history of TB epidemics, including emergence of HIV and MDR TB in the second half of the 20th century, has taught us that professional and economic isolation are dangerous co-conspirators. Control of TB in the antibiotic era requires coordinated international approaches to upgrade laboratory infrastructure, manage global drug supplies, and support research for new diagnostics, drugs, and vaccines. Academic collaborations with the DPRK focused on TB research and control offer important, ideologically neutral opportunities for assimilation within the international health and related scientific research community. Through the World STOP TB partnership, the American-Thoracic Society, the U.S. CDC, and the International Union against Tuberculosis and Lung Disease, the international TB professional community has developed an extensive global network of training, consultancy, and quality assessment resources. Providing opportunities for North Korean public health officials to link to this dynamic pedagogic community should be a priority. The establishment of a reference-level national TB laboratory in the DPRK also begins to address an important blind spot in TB control for Northeast Asia. The laboratory can serve as a basis to foster new professional relations applied to regional disease surveillance, infrastructure development, innovative professional practices, and other technical assistance exchanges.
24
2012 Volume 5
ON KOREA
Regional partnerships, such as the Middle East Consortium on Infectious Disease Surveillance and the Mekong Basin Disease Surveillance Network, show that such engagements are possible despite the lack of diplomatic relations among member countries.73 Other regions of the world that would benefit from regional planning for TB control include the Eurasian arc encompassing Afghanistan to Pakistan, India, and the southern republics of the former Soviet Union, and the cluster of countries in Southeast Asia. For political reasons similar to those affecting Northeast Asia, countries in these clusters report to different WHO regional headquarters. In contrast with the situation 25 years ago, the world is in a far better position today to recognize the risks of MDR TB epidemics where food and TB drug shortages persist. Although substantial resources are now available to respond to MDR TB hot spots, the TB epidemic in North Korea illustrates that these mechanisms still do not work well in non-treaty areaswhere, nonetheless, they may be most needed. First, in regions isolated by conflict, epidemiologic trends are often difficult to track or the documentation simply does not exist. Second, high-level political agreements needed to engage in regional planning and to implement critical assistance programs may not be possible. Third, food, immunization, and energy shortages, typically not embraced as TB program assistance, are part of weakened public health systems and need to be addressed by international TB response systems. Finally, policy, humanitarian, and medical communities need to work creatively together to structure the opportunities that lead to constructive, sustained engagement in areas isolated by conflict. For these reasons, private initiatives such as ours remain vital to extend the frontiers of global TB control efforts. Our project worked within an existing bureaucratic structure that is unique to the history of TB assistance for the DPRK. For these efforts to translate into broader engagement opportunities for U.S. academic institutions, additional education is needed. At the present time, the primary point of access for university engagement is through the Korean-American Private Exchange Society (KAPES), a self-described nonprofit North Korean entity established in 2005 and charged with managing U.S.-based humanitarian and academic relationships. This structure faces limitations in introducing the extraordinary range of intellectual resources that U.S. universities can bring to academic collaborations with North Korean scientists.74 Recent efforts like the U.S.-DPRK Scientific Exchange Consortium75 are important not only to educate North Korea about the organization of higher education and research in the United States but also to promote a coordinated approach to academic engagement on the U.S. side.
Perry, Linton, Gresham, and Schoolnik: Engaging North Korea
25
Summary and Conclusions
Historically, health assistance has been relegated to the role of humanitarian effort and has occupied a subordinate role in foreign policy. With globalization and the emergence of shared threats such as HIV, MDR TB, avian influenza, and bioterrorism, health and security policy are increasingly connected.76 As one of the last outposts of Cold War politics,77 the 60-year-old Korean conflict challenges us to recognize this connection. While media coverage of North Korea remains dominated by conventional security concerns, U.S. citizens, including more than two million ethnic Koreans, are increasingly aware of the economic rigors faced by the North Korean people.78 As some observers are suggesting,79 economic sanctions intended to induce the DPRK to abandon its nuclear weapons programs may be untenable from both security and humanitarian perspectives. In this view, by greatly discouraging foreign private sector participation, economic sanctions have had the unintended effect of exacerbating a public health crisis in the DPRK. Tuberculosis trends, a barometer that touches every aspect of human health, illustrate the deadly externalities of this approach. Our experience shows that constructive health engagements with the DPRK are possible despite diplomatic reversals at the state-to-state level. A review of sanctions policies with the aim of facilitating broader public health engagements, like the U.S.-DPRK Tuberculosis Project, is urgently needed for humanitarian reasons. In the longer term, expanded public health exchanges may also contribute to the reduction of tensions on the Korean Peninsula and a positive evolution of relations with the DPRK. Sharon Perry served as director of the Stanford DPRK TB Laboratory Project from 2008 to 2011, and is a member of the National Committee on North Korea. Gary Schoolnik is associate dean and professor of medicine at Stanford University School of Medicine, Stanford, California; Heidi Linton is executive director of Christian Friends of Korea, Black Mountain, North Carolina; and Louise Gresham is director of the Global Health and Security Initiative, Nuclear Threat Initiative, Washington, D.C. The authors gratefully acknowledge the Stanford/BATC laboratory advisory and training teams, including Dr. Ed Desmond, Dr. Niaz Banaei, Ms. Grace Lin, Ms. Linda Kuo, Dr. Robert Luo, and Dr. James MacLaughlin as well as CFK clinical laboratory expert Dr. Marcia Kilsby of Andrews University, CFK microbiologist Dr. Choong Park, CFK construction engineer Mr. Rob Robinson, CFK bioengineer Mr. Mark Heydenburg, and more than a dozen skilled volunteer tradesmen. The authors thank Mr. David Straub for his valuable comments on the manuscript.
26
2012 Volume 5
ON KOREA
References
1 R. Carlin and J. W. Lewis, North Koreas New Course, Los Angeles Times, 8 December 2011. 2 S. S. Hecker, Lessons Learned from the North Korean Nuclear Crises, Daedulus (Winter 2010): 4456. 3 J. Owen-Davies, North Koreas Public Health Tragedy, Lancet 357 (2000): 62830; S. Haggard and M. Noland, Famine in North Korea: Markets, Aid and Reform (New York: Columbia University, 2007). 4 S. Perry, H. Linton, and G. K. Schoolnik, Tuberculosis in North Korea, Science (New York) 331 (2011): 263. 5 M. Manyin and M. B. Nikitin, Foreign Assistance to North Korea (Washington, D.C.: Congressional Research Service, 2010). 6 Talking to North Korea (editorial), New York Times, 13 January 2011; J. W. Lewis and R. Carlin, Review U.S. Policy toward North Korea, Washington Post, 22 November 2010. 7 R. Stone, New Tuberculosis Laboratory Hailed as Break-Through in Health Diplomacy, Science (New York) 327 (2010): 131213; A. Gee, U.S. and North Korea Work Together on Tuberculosis, Lancet 375 (2010): 1862; D. G. McNeil Jr., Tuberculosis: North Korea Develops TB Laboratory with Help from American Doctors, New York Times, 1 March 2010. 8 WHO, Global Tuberculosis Control 2010 (Geneva: World Health Organization, 2010). 9 R. Baltussen, K. Floyd, and C. Dye, Cost-Effectiveness Analysis of Strategies for Tuberculosis Control in Developing Countries, BMJ 331 (2005): 1364; R. Laxminarayan et al., Economic Benefits of Tuberculosis Control (policy working paper, World Bank, Washington, D.C., August 2007). 10 R. Hershberg et al., High Functional Diversity in Mycobacterium Tuberculosis Driven by Genetic Drift and Human Demography, PLoS biology 6 (2008): e311. 11 G. W. Comstock and G. M. Cauthen, Epidemiology of Tuberculosis, in Tuberculosis: A Comprehensive Approach, ed. L. Reichman and E. Herschfield, 2348 (New York: Marcel Decker, 1993); P. L. Lin and J. L. Flynn, Understanding Latent Tuberculosis: A Moving Target, J Immunol 185 (2010): 1522. 12 WHO, Global Tuberculosis Control: Epidemiology, Strategy, Financing, report no. WHO/HTM/TB/2009.411 (Geneva: World Health Organization, 2009). [Author: This is the title of the publication with this report number.] 13 R. Fortuine, Why Must We All Die: Alaskas Enduring Struggle with Tuberculosis (Anchorage: University of Alaska, 2005). 14 P. C. Hopewell, M. Pai, D. Maher, M. Uplekar, and M. C. Raviglione, International Standards for Tuberculosis Care, Lancet Infectious Diseases 6 (2006): 71025; American Thoracic Society, Centers for Disease Control and Prevention, Infectious Diseases Society of America: Controlling Tuberculosis in the United States, American Journal of Respiratory and Critical Care Medicine 172 (2005): 11691227; WHO, Treatment of Tuberculosis: Guidelines, 4th ed. (Geneva: World Health Organization, 2009). Drug-susceptible disease is treated with four or five standard first-line anti-TB drugs; second-line drugs for treatment of drug-resistant TB include several additional antibiotics. 15 WHO, Global Tuberculosis Control 2010. 16 Centers for Disease Control and Prevention, Reported Tuberculosis Cases in the United States, 2009, www.cdc.gov/tb/. 17 E. L. Corbett et al., The Growing Burden of Tuberculosis: Global Trends and Interactions with the HIV Epidemic, Archives of Internal Medicine 163 (2003): 100921. 18 D. E. Snider Jr. and K. G. Castro, The Global Threat of Drug-Resistant Tuberculosis, New England Journal of Medicine 338 (1998): 168990.
Perry, Linton, Gresham, and Schoolnik: Engaging North Korea
27
19 WHO, Multidrug and Extensively Drug-Resistant TB (M/XDR-TB): 2010 Global Report on Surveillance and Response, report no. WHO/HTM/TB/2010.3 (Geneva: World Health Organization, 2010); N. R. Gandhi et al., Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis: A Threat to Global Control of Tuberculosis, Lancet 375 (2010): 183043. 20 S. Keshavjee and P. E. Farmer, Picking Up the PaceScale-Up of MDR Tuberculosis Treatment Programs, New England Journal of Medicine 363 (2010): 178184. 21 WHO, Multidrug and Extensively Drug-Resistant TB (M/XDR-TB). 22 Gandhi et al., Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis; P. R. Donald and P. D. van Helden, The Global Burden of TuberculosisCombating Drug Resistance in Difficult Times, New England Journal of Medicine 360 (2009): 239395. 23 WHO, Multidrug and Extensively Drug-Resistant TB (M/XDR-TB). 24 Up to 10 percent of MDR cases are thought to affect children under the age of 15. Tuberculosis in a young child is both difficult to diagnose and a sentinel of community transmission; see, for example, H. S. Schaaf, B. J. Marais, A. C. Hesseling, W. Brittle, and P. R. Donald, Surveillance of Antituberculosis Drug Resistance among Children from the Western Cape Province of South AfricaAn Upward Trend, American Journal of Public Health 99 (2009): 148690. 25 Gandhi et al., Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis. 26 A. Wright et al., Epidemiology of Antituberculosis Drug Resistance 200207: An Updated Analysis of the Global Project on Anti-Tuberculosis Drug Resistance Surveillance, Lancet 373 (2009) 186173. 27 WHO, Multidrug and Extensively Drug-Resistant TB (M/XDR-TB); S. Toungoussova, D. A. Caugant, P. Sandven, A. O. Mariandyshev, and G. Bjune, Drug Resistance of Mycobacterium Tuberculosis Strains Isolated from Patients with Pulmonary Tuberculosis in Archangels, Russia, Int J Tuberc Lung Dis 6 (2002): 40614. 28 WHO, Multidrug and Extensively Drug-Resistant TB (M/XDR-TB). 29 O. S. Toungoussova, G. Bjune, and D. A. Caugant, Epidemic of Tuberculosis in the Former Soviet Union: Social and Biological Reasons, Tuberculosis (Edinb) 86 (2006): 110; D. Stuckler, S. Basu, M. McKee, and L. King, Mass Incarceration Can Explain Population Increases in TB and Multidrug-Resistant TB in European and Central Asian Countries, Proceedings of the National Academy of Sciences of the United States of America 105 (2008): 13280285 (2008). 30 P. J. Bifani, B. Mathema, N. E. Kurepina, and B. N. Kreiswirth, Global Dissemination of the Mycobacterium Tuberculosis W-Beijing Family Strains, Trends Microbiol 10 (2002): 4552; I. Mokrousov et al., Origin and Primary Dispersal of the Mycobacterium Tuberculosis Beijing Genotype: Clues from Human Phylogeography, Genome Research 15 (2005): 135764; E. Lasunskaia et al., Emerging Multidrug Resistant Mycobacterium Tuberculosis Strains of the Beijing Genotype Circulating in Russia Express a Pattern of Biological Properties Associated with Enhanced Virulence, Microbes Infect 12 (2010): 46775; J. R. Glynn, K. Kremer, M. P. Rodrigues, and D. van Soolingen, Beijing/W Genotype Mycobacterium tuberculosis and Drug Resistance, Emerging Infectious Diseases 12 (2006): 73643; D. Cowley et al., Recent and Rapid Emergence of W-Beijing Strains of Mycobacterium Tuberculosis in Cape Town, South Africa, Clin Infect Dis 47 (2008): 125259; T. Kubica, S. Rusch-Gerdes, and S. Niemann, The Beijing Genotype Is Emerging among Multidrug-Resistant Mycobacterium Tuberculosis Strains from Germany, Int J Tuberc Lung Dis 8 (2004): 110713. 31 P. M. Small and M. Pai, Tuberculosis DiagnosisTime for a Game Change, New England Journal of Medicine 363 (2010): 107071. 32 Donald and van Helden, The Global Burden of Tuberculosis. 33 WHO, Multidrug and Extensively Drug-Resistant TB (M/XDR-TB), 2011. 34 R. Gupta et al., Increasing Transparency in Partnerships for HealthIntroducing the Green Light Committee, Trop Med Int Health 7 (2002): 97076.
28
2012 Volume 5
ON KOREA
35 A. Laszlo, M. Rahman, M. Espinal, and M. Raviglione, Quality Assurance Programme for Drug Susceptibility Testing of Mycobacterium Tuberculosis in the WHO/IUATLD Supranational Reference Laboratory Network: Five Rounds of Proficiency Testing, 19941998, Int J Tuberc Lung Dis 6 (2002): 74856. 36 S. Keshavjee and P. E. Farmer, Picking Up the Pace. 37 WHO, Health in Asia and the Pacific (New Delhi: WHO Regional Office of Southeast Asia, 2008); Organization for Economic Cooperation and Development, Health at a Glance, Asia-Pacific 2010 (OECD, 2010); S. Perry, Health Care Infrastructure Challenges in DPRK (presentation at USC-Center for Strategic and International Studies conference, August 2011). 38 WHO, WHO Country Cooperation Strategy, 20042008: Democratic Peoples Republic of North Korea (Pyongyang Office and Geneva: World Health Organization, 2003). Other ministries, including the military, railways, and prisons, also operate health care systems. 39 R. Weitz, Russia and the Koreas: Past Policies and Future Possibilities, Academic Paper Series on Korea (Korea Economic Institute) 5 (2010): 117. 40 As an artifact of the Korean conflict, the DPRK is assigned to the South East Region of WHO operations headquartered in New Delhi, while South Korea (and also China) is assigned to the Western Pacific Region, headquartered in Manila. 41 WHO, WHO Country Cooperation Strategy, 20042008; D. Goodkind and L. West, The North Korean Famine and Its Demographic Impact, Population and Development Review (2001). 42 WHO, Global Tuberculosis Control: Country Data, World Health Organization, Geneva, 2010. 43 WHO, Health in Asia and the Pacific; OECD, Health at a Glance. Average caloric intake for the Asia-Pacific region was estimated at 2500 k/cal in 2007 (Food and Agriculture Organization, faostat.org, cited in OECD, Health at a Glance). The 2009 WFP/FAO/UNICEF Crop and Food Security Assessment used a baseline of 1640 k/cal for North Korea. 44 Institute of Children Nutrition, DPRK 2004 Nutrition Survey: Report of Survey Results (Pyongyang, DPRK, 2005). 45 North Koreans Life Expectancy Falls as Infant Mortality Rises, The Times (London), 22 February 2010. 46 WHO, WHO Country Cooperation Strategy, 20042008. 47 DOTS focuses on patient adherence to a course of treatment and is thus a strategic prevention program for MDR TB. 48 WHO, DPRK: Country Profile, World Health Organization, Geneva, 2006. 49 WHO, The Regional Strategic Plan for Tuberculosis Control 20062015 (New Delhi: World Health Organization, Regional Office for Southeast Asia, 2006). 50 WHO, Global Tuberculosis Control: Country Data; WHO, Democratic Peoples Republic of Korea: Tuberculosis Profile, 2009, www.who.int/tb/data. 51 Sarveshwar Puri, personal communication with author; meeting at WHO Country Office with representatives of the U.S.-DPRK Tuberculosis Project, Pyongyang, 25 April 2010. 52 WHO, Global Tuberculosis Control 2010. 53 WHO, Global Tuberculosis Control: Country Data. 54 WHO, DPRK: Country Profile, 2010. 55 WHO, The Regional Strategic Plan for Tuberculosis Control 20062015. 56 According to WHO Country Profile, 2009, HIV infection is not considered a factor in the DPRK TB epidemic.
Perry, Linton, Gresham, and Schoolnik: Engaging North Korea
29
57 Christian Friends of Korea and the Eugene Bell Foundation have provided supplemental drugs as well as food and agricultural and other supplies to TB facilities largely in the four westernmost provinces of the DPRK since 1997. 58 WHO and MoPH officials, personal communication to members of the Stanford/BATC, 14 January 2008; U.S. food aid to the DPRK dropped to nothing in fiscal years 2006 and 2007, and in 2008 the United States terminated new shipments through the World Food Programme owing to disagreements over verification; see Foreign Assistance to North Korea (Washington, D.C.: Congressional Research Office, 12 March 2010). 59 UNICEF, Strengthening Tuberculosis Control in DPR Korea, Global Fund to Fight AIDS, Tuberculosis and Malaria, North Korea, 2010. In 2012, DPRK plans to apply for a continuation of its Global Fund award through 2014; like many countries entering continuation phase, cuts are expected owing to donor replenishment shortfalls. 60 Ibid. 61 WHO, Global Tuberculosis Control; J. Parry, North Koreas Fight against Tuberculosis Gets a Boost, BMJ (Clinical research ed) 340 (2010): c2223. 62 G. X. He et al., Prevalence of Tuberculosis Drug Resistance in 10 Provinces of China, BMC Infectious Diseases 8 (2008): 166. 63 WHO, Multidrug and Extensively Drug-Resistant TB (M/XDR-TB); G. Tsogt et al., Nationwide Tuberculosis Drug Resistance Survey in Mongolia, 1999, Int J Tuberc Lung Dis 6 (2002): 28994. 64 G.X. He et al., Availability of Second-Line Drugs and Anti-Tuberculosis Drug Susceptibility Testing in China: A Situational Analysis, Int J Tuberc Lung Dis 14 (2010): 88489. 65 Gandhi et al., Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis. 66 WHO, Multidrug and Extensively Drug-Resistant TB (M/XDR-TB). 67 Gandhi et al., Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis. 68 E. Cody, Tentative Nuclear Deal Struck with North Korea, Washington Post, 13 February 2007; J. W. Lewis and R. Carlin, What North Korea Really Wants, Washington Post, 27 January 2007. 69 WHO, Regional Strategic Plan for Tuberculosis Control 20062015. 70 WHO, Guidelines for Surveillance of Drug Resistance in Tuberculosis, 4th ed. (Geneva: World Health Organization, 2009). 71 WHO, Treatment of Tuberculosis: Guidelines, 4th ed. 72 L. Gresham, A. Ramlawi, J. Briski, M. Richardson, and T. Taylor, Trust across Borders: Responding to 2009 H1N1 Influenza in the Middle East, Biosecurity and Bioterrorism: Biodefense, Strategy, Practice, and Science 7 (2009) 399404. 73 Ibid. 74 Sharon Perry, The Stanford North Korean Tuberculosis Project, in U.S.-DPRK Educational Exchanges: Assessment and Future Strategy, ed. Gi-wook Shin and Karin J. Lee (Stanford: Walter H. Shorenstein Asian Pacific Research Center, Stanford University, 2011). 75 H. Seo and S. Thorson, Academic Science Engagement with North Korea, Academic Paper Series on Korea (Korea Economic Institute) 3 (2010): 10521; P. C. Agre and V. Turekian, Advancing Science, Promoting Peace, Science Translational Medicine 2 (2010): 12. 76 D. P. Fidler, Health as Foreign Policy: Harnessing Globalization for Health, Health Promotion International 21 (2007): 5158. 77 F. Gavin, Same as It Ever Was: Nuclear Alarmism, Proliferation and the Cold War, International Security 34 (2009): 737. 78 Barbara Demick, Nothing to Envy: Ordinary Lives in North Korea (New York: Speigel & Grau, 2009). 79 Lewis and Carlin, Review U.S. Policy toward North Korea.
30
2012 Volume 5
ON KOREA
On Korea began in December 2006 with the initiation of KEIs Academic Paper Series, a year-long program that provides both leading Korea scholars and new voices from around the world to speak and write on current events and trends on the Korean peninsula. Each year, KEI commissions approximately ten papers and distributes them individually to over 5,000 government officials, think tank experts, and scholars around the United States and the world. Authors are invited to the Korea Economic Institute to discuss their research before a Washington, DC policy audience. At the conclusion of each series, the papers are n compiled and published together as the On Korea volume. To learn more about how to contribute to future Academic Papers Series forums and other programs at KEI, please visit: www.keia.org.
Authors:
John Everard Jos Luis Len-Manrquez ez Yeongkwan Song g Yoon-shik Park -shik Michael J. Mazarr and the Study Group on North Korean Futures Balbina Y. Hwang Abraham M. Denmark Sharon Perry, Heidi Linton, Louise Gresham, and Gary Schoolnik Duyeon Kim
Korea Economic Institute of America 1800 K St. NW, Suite 1010, Washington, DC 20006 P.202.464.1982 F.202.464.1987 www.keia.org
Вам также может понравиться
- Narratives of Civic Duty: How National Stories Shape Democracy in AsiaОт EverandNarratives of Civic Duty: How National Stories Shape Democracy in AsiaОценок пока нет
- A Year in PyongyangДокумент129 страницA Year in PyongyangDana CoeОценок пока нет
- Introduction To Survival Analysis With Stata SeminarДокумент16 страницIntroduction To Survival Analysis With Stata Seminarhubik38Оценок пока нет
- Demographic TransitionДокумент5 страницDemographic TransitionreddishpinkОценок пока нет
- The Myth of Triumphalism: Rethinking President Reagan's Cold War LegacyОт EverandThe Myth of Triumphalism: Rethinking President Reagan's Cold War LegacyОценок пока нет
- Hettne, Development of Development TheoryДокумент21 страницаHettne, Development of Development TheoryVer Madrona Jr.Оценок пока нет
- Project 1: Analyze The Rhetorical Situation in A Set of TextsДокумент3 страницыProject 1: Analyze The Rhetorical Situation in A Set of TextsAkksay SinghОценок пока нет
- The Secret Syllabus: A Guide to the Unwritten Rules of College SuccessОт EverandThe Secret Syllabus: A Guide to the Unwritten Rules of College SuccessОценок пока нет
- Survival Analysis in RДокумент16 страницSurvival Analysis in Rmipimipi03Оценок пока нет
- It's Madness: The Politics of Mental Health in Colonial KoreaОт EverandIt's Madness: The Politics of Mental Health in Colonial KoreaОценок пока нет
- Reimagining Global HealthДокумент5 страницReimagining Global HealthMariela Planas100% (1)
- Gerontology Chapter 1 IntroДокумент9 страницGerontology Chapter 1 IntroSJОценок пока нет
- J.olsen The Many Faces of EuropeanizationДокумент32 страницыJ.olsen The Many Faces of EuropeanizationBetka RemiasovaОценок пока нет
- Biostatistics and Computer-based Analysis of Health Data using RОт EverandBiostatistics and Computer-based Analysis of Health Data using RОценок пока нет
- Depression in Caged Animals: A Study at The National Zoo, Kuala Lumpur, MalaysiaДокумент12 страницDepression in Caged Animals: A Study at The National Zoo, Kuala Lumpur, MalaysiaSilvina PezzettaОценок пока нет
- The Uncertain Legacy of Crisis: European Foreign Policy Faces the FutureОт EverandThe Uncertain Legacy of Crisis: European Foreign Policy Faces the FutureОценок пока нет
- MethdologyДокумент41 страницаMethdologyasmeraamde21Оценок пока нет
- Barefoot Global Health Diplomacy: Field Experiences in International Relations, Security, and EpidemicsОт EverandBarefoot Global Health Diplomacy: Field Experiences in International Relations, Security, and EpidemicsОценок пока нет
- Reducing Screen-Time and UnhealthyДокумент14 страницReducing Screen-Time and UnhealthyJohana Vangchhia100% (1)
- AEFI Surveillance and Response Operational Guidelines 2015Документ204 страницыAEFI Surveillance and Response Operational Guidelines 2015anunad100% (1)
- Walker - A BIOARCHAEOLOGICAL PERSPECTIVE ON THE HISTORY OF VIOLENCEДокумент30 страницWalker - A BIOARCHAEOLOGICAL PERSPECTIVE ON THE HISTORY OF VIOLENCELuis Lobato de Faria100% (2)
- Global "Body Shopping": An Indian Labor System in the Information Technology IndustryОт EverandGlobal "Body Shopping": An Indian Labor System in the Information Technology IndustryОценок пока нет
- Daly Text 9x6 PDFДокумент58 страницDaly Text 9x6 PDFChad ThompsonОценок пока нет
- Outsourcing War: The Just War Tradition in the Age of Military PrivatizationОт EverandOutsourcing War: The Just War Tradition in the Age of Military PrivatizationРейтинг: 4 из 5 звезд4/5 (1)
- Measuring The Global Burden of DiseaseДокумент10 страницMeasuring The Global Burden of DiseaseLili CRОценок пока нет
- The Nativist Lobby: Three Faces of IntoleranceДокумент21 страницаThe Nativist Lobby: Three Faces of IntoleranceBento Spinoza100% (1)
- The Reshaped Economic Relations Between Russia and Turkey After Western Economic SanctionsОт EverandThe Reshaped Economic Relations Between Russia and Turkey After Western Economic SanctionsОценок пока нет
- M.Sc. Dissertation.Документ92 страницыM.Sc. Dissertation.Oladeji OlayideОценок пока нет
- 2011 The Immune Hallmarks of CancerДокумент8 страниц2011 The Immune Hallmarks of CancerCristian Gutiérrez VeraОценок пока нет
- China's New Diplomacy Concept: Building a Community of Shared Future for MankindОт EverandChina's New Diplomacy Concept: Building a Community of Shared Future for MankindОценок пока нет
- The Ethnic Conflict in Sri Lanka - A Historical and Sociopolitical Outline - Sasanka PereraДокумент29 страницThe Ethnic Conflict in Sri Lanka - A Historical and Sociopolitical Outline - Sasanka PereraSarawananNadarasaОценок пока нет
- The Instrumental University: Education in Service of the National Agenda after World War IIОт EverandThe Instrumental University: Education in Service of the National Agenda after World War IIОценок пока нет
- Thailand Health Profile Report 2008-2010Документ12 страницThailand Health Profile Report 2008-2010Oon KooОценок пока нет
- Truthfulness and RelevanceДокумент51 страницаTruthfulness and RelevanceWes Siscoe100% (1)
- Refugees and the Transformation of Societies: Agency, Policies, Ethics and PoliticsОт EverandRefugees and the Transformation of Societies: Agency, Policies, Ethics and PoliticsОценок пока нет
- Under Watch - Reporting in China's Surveillance StateДокумент17 страницUnder Watch - Reporting in China's Surveillance StateJojje OlssonОценок пока нет
- Our Latest Longest War: Losing Hearts and Minds in AfghanistanОт EverandOur Latest Longest War: Losing Hearts and Minds in AfghanistanОценок пока нет
- Global Burden of Disease GBD Study 2017 18 PDFДокумент70 страницGlobal Burden of Disease GBD Study 2017 18 PDFtutagОценок пока нет
- Developing Country Debt and Economic Performance, Volume 1: The International Financial SystemОт EverandDeveloping Country Debt and Economic Performance, Volume 1: The International Financial SystemОценок пока нет
- Stereotype Threat With VideoДокумент18 страницStereotype Threat With VideoweigansmОценок пока нет
- TOEFL iBT Premium with 8 Online Practice Tests + Online Audio, Eighteenth EditionОт EverandTOEFL iBT Premium with 8 Online Practice Tests + Online Audio, Eighteenth EditionОценок пока нет
- Burma/Myanmar: Outside Interests and Inside Challenges, Outside InterestsДокумент234 страницыBurma/Myanmar: Outside Interests and Inside Challenges, Outside Interestsrohingyablogger100% (1)
- Iraq at a Distance: What Anthropologists Can Teach Us About the WarОт EverandIraq at a Distance: What Anthropologists Can Teach Us About the WarОценок пока нет
- LSE For You - Candidate Number and Exam TimetableДокумент2 страницыLSE For You - Candidate Number and Exam TimetablediyaОценок пока нет
- Muslim, Trader, Nomad, Spy: China's Cold War and the People of the Tibetan BorderlandsОт EverandMuslim, Trader, Nomad, Spy: China's Cold War and the People of the Tibetan BorderlandsОценок пока нет
- Oregon - 5Документ2 страницыOregon - 5Korea Economic Institute of America (KEI)Оценок пока нет
- Tennessee - 7Документ2 страницыTennessee - 7Korea Economic Institute of America (KEI)Оценок пока нет
- Fundamental Theories of Ethnic Conflict: Explaining the Root Causes of Ethnic and Racial HateОт EverandFundamental Theories of Ethnic Conflict: Explaining the Root Causes of Ethnic and Racial HateОценок пока нет
- Ohio - 12Документ2 страницыOhio - 12Korea Economic Institute of America (KEI)Оценок пока нет
- Economic and Political Reform in Africa: Anthropological PerspectivesОт EverandEconomic and Political Reform in Africa: Anthropological PerspectivesОценок пока нет
- Ohio - 7Документ2 страницыOhio - 7Korea Economic Institute of America (KEI)Оценок пока нет
- From Convergence to Crisis: Labor Markets and the Instability of the EuroОт EverandFrom Convergence to Crisis: Labor Markets and the Instability of the EuroОценок пока нет
- Ohio - 10Документ2 страницыOhio - 10Korea Economic Institute of America (KEI)Оценок пока нет
- India and the Patent Wars: Pharmaceuticals in the New Intellectual Property RegimeОт EverandIndia and the Patent Wars: Pharmaceuticals in the New Intellectual Property RegimeОценок пока нет
- Connecticut - 1Документ2 страницыConnecticut - 1Korea Economic Institute of America (KEI)Оценок пока нет
- Florida - 25Документ2 страницыFlorida - 25Korea Economic Institute of America (KEI)Оценок пока нет
- Ohio - 6Документ2 страницыOhio - 6Korea Economic Institute of America (KEI)Оценок пока нет
- Ohio - 1Документ2 страницыOhio - 1Korea Economic Institute of America (KEI)Оценок пока нет
- Ohio - 4Документ2 страницыOhio - 4Korea Economic Institute of America (KEI)Оценок пока нет
- Top FL-17th Export of Goods To Korea in 2016Документ2 страницыTop FL-17th Export of Goods To Korea in 2016Korea Economic Institute of America (KEI)Оценок пока нет
- Top TX-17th Export of Goods To Korea in 2016Документ2 страницыTop TX-17th Export of Goods To Korea in 2016Korea Economic Institute of America (KEI)Оценок пока нет
- Top CA-34th Export of Goods To Korea in 2016Документ2 страницыTop CA-34th Export of Goods To Korea in 2016Korea Economic Institute of America (KEI)Оценок пока нет
- Top CA-13th Export of Goods To Korea in 2016Документ2 страницыTop CA-13th Export of Goods To Korea in 2016Korea Economic Institute of America (KEI)Оценок пока нет
- Top TX-19th Export of Goods To Korea in 2016Документ2 страницыTop TX-19th Export of Goods To Korea in 2016Korea Economic Institute of America (KEI)Оценок пока нет
- Top TX-30th Export of Goods To Korea in 2016Документ2 страницыTop TX-30th Export of Goods To Korea in 2016Korea Economic Institute of America (KEI)Оценок пока нет
- Texas - 35 - UpdatedДокумент2 страницыTexas - 35 - UpdatedKorea Economic Institute of America (KEI)Оценок пока нет
- Maryland - 6Документ2 страницыMaryland - 6Korea Economic Institute of America (KEI)Оценок пока нет
- Washington - 1Документ2 страницыWashington - 1Korea Economic Institute of America (KEI)Оценок пока нет
- Georgia - 9Документ2 страницыGeorgia - 9Korea Economic Institute of America (KEI)Оценок пока нет
- Oregon - 4Документ2 страницыOregon - 4Korea Economic Institute of America (KEI)Оценок пока нет
- Utah - 2Документ2 страницыUtah - 2Korea Economic Institute of America (KEI)Оценок пока нет
- Arizona - 3Документ2 страницыArizona - 3Korea Economic Institute of America (KEI)Оценок пока нет
- Utah - 3Документ2 страницыUtah - 3Korea Economic Institute of America (KEI)Оценок пока нет
- Top AR-3rd Export of Goods To Korea in 2016Документ2 страницыTop AR-3rd Export of Goods To Korea in 2016Korea Economic Institute of America (KEI)Оценок пока нет
- Florida - 2Документ2 страницыFlorida - 2Korea Economic Institute of America (KEI)Оценок пока нет
- Top OH-9th Export of Goods To Korea in 2016Документ2 страницыTop OH-9th Export of Goods To Korea in 2016Korea Economic Institute of America (KEI)Оценок пока нет
- Florida - 14Документ2 страницыFlorida - 14Korea Economic Institute of America (KEI)Оценок пока нет
- Top AL-4th Export of Goods To Korea in 2016Документ2 страницыTop AL-4th Export of Goods To Korea in 2016Korea Economic Institute of America (KEI)Оценок пока нет
- North Carolina - 1Документ2 страницыNorth Carolina - 1Korea Economic Institute of America (KEI)Оценок пока нет
- Ipi 262542Документ6 страницIpi 262542elsi mindahaОценок пока нет
- Panchagavya (Uses Benefits and Preparation)Документ16 страницPanchagavya (Uses Benefits and Preparation)Shreya VermaОценок пока нет
- Diagnosing TB: Old and New Tools (Dr. Anne Detjen)Документ56 страницDiagnosing TB: Old and New Tools (Dr. Anne Detjen)National Press Foundation100% (1)
- Updatesinpediatric Tuberculosisin Internationalsettings: Sadia Shakoor,, Fatima MirДокумент27 страницUpdatesinpediatric Tuberculosisin Internationalsettings: Sadia Shakoor,, Fatima MirCamilo TobonОценок пока нет
- Bureau of Customs CMO-28-2017Документ1 страницаBureau of Customs CMO-28-2017PortCallsОценок пока нет
- Paper Cutting 6Документ71 страницаPaper Cutting 6Vidya AdsuleОценок пока нет
- Pending 2Документ2 страницыPending 2Ma. Alexis DiezmoОценок пока нет
- Coc Project L - IVДокумент12 страницCoc Project L - IVDaanGutuHumnasaОценок пока нет
- AlereДокумент6 страницAlereDarryl John PasambaОценок пока нет
- Health PlanningДокумент7 страницHealth PlanningPaulОценок пока нет
- Firs World Report PDFДокумент35 страницFirs World Report PDFMarv MarvОценок пока нет
- Self Assessment ToolДокумент25 страницSelf Assessment ToolJoylyn Mendez LlenaОценок пока нет
- Infectious Diseases IIДокумент57 страницInfectious Diseases IIAhmad MakhloufОценок пока нет
- 2013 Manual of Procedures For The National TB Control ProgramДокумент134 страницы2013 Manual of Procedures For The National TB Control ProgramCarlo Giorgio DC CerezoОценок пока нет
- Risk Assessment Guidelines For Diseases Transmitted On AircraftДокумент41 страницаRisk Assessment Guidelines For Diseases Transmitted On AircraftAndrei MuresanОценок пока нет
- Drug Development Against Tuberculosis Impact of AlkaloidsДокумент41 страницаDrug Development Against Tuberculosis Impact of Alkaloidsamine ben dahsenОценок пока нет
- The New York Times International (16.08.19)Документ16 страницThe New York Times International (16.08.19)Rita de Cassia OfranteОценок пока нет
- Astigmidwife Vlogs Online Tutorial: All Rights Are Reserved. No Part of This Publication May Be ReproducedДокумент12 страницAstigmidwife Vlogs Online Tutorial: All Rights Are Reserved. No Part of This Publication May Be ReproducedLynden BulanОценок пока нет
- Chapter 1 Communicable Diseases 2ND Sem 2022 2023Документ10 страницChapter 1 Communicable Diseases 2ND Sem 2022 2023Lovelyn Cantollas EugenioОценок пока нет
- Dukungan Keluarga Sebagai Faktor Penting Dalam Kepatuhan Minum Obat Pada Pasien Tuberkulosis ParuДокумент7 страницDukungan Keluarga Sebagai Faktor Penting Dalam Kepatuhan Minum Obat Pada Pasien Tuberkulosis ParuRiki Permana PutraОценок пока нет
- Cambridge International AS & A Level: Biology 9700/12Документ16 страницCambridge International AS & A Level: Biology 9700/12lllllisaОценок пока нет
- The Untilled Fields of Public Health PDFДокумент11 страницThe Untilled Fields of Public Health PDFFotis PerdikoulisОценок пока нет
- Thesis DoneДокумент24 страницыThesis DoneAmira SaidinОценок пока нет
- Nigeria: Federal Ministry of Health's Health Promotion PolicyДокумент27 страницNigeria: Federal Ministry of Health's Health Promotion PolicyState House NigeriaОценок пока нет
- (1922) The Story of A National CrimeДокумент32 страницы(1922) The Story of A National CrimeHerbert Hillary Booker 2ndОценок пока нет
- Pediatric PneumoniaДокумент12 страницPediatric PneumoniaKrystal Migo Denolo ContrerasОценок пока нет
- School TB Case Letterhead 12.29.16Документ2 страницыSchool TB Case Letterhead 12.29.16Hank LeeОценок пока нет
- Topic 13 Global Distribution of Diseases My NC Notes 1Документ31 страницаTopic 13 Global Distribution of Diseases My NC Notes 1Melogina ManoОценок пока нет
- Social Determinants of HealthДокумент27 страницSocial Determinants of HealthDensearn Seo100% (5)
- Health, History and Hard Choices: Funding Dilemmas in A Fast - Changing WorldДокумент26 страницHealth, History and Hard Choices: Funding Dilemmas in A Fast - Changing WorldAbdiwaliОценок пока нет
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (34)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- The War after the War: A New History of ReconstructionОт EverandThe War after the War: A New History of ReconstructionРейтинг: 5 из 5 звезд5/5 (2)
- Son of Hamas: A Gripping Account of Terror, Betrayal, Political Intrigue, and Unthinkable ChoicesОт EverandSon of Hamas: A Gripping Account of Terror, Betrayal, Political Intrigue, and Unthinkable ChoicesРейтинг: 4.5 из 5 звезд4.5/5 (506)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (46)
- Briefly Perfectly Human: Making an Authentic Life by Getting Real About the EndОт EverandBriefly Perfectly Human: Making an Authentic Life by Getting Real About the EndОценок пока нет
- Age of Revolutions: Progress and Backlash from 1600 to the PresentОт EverandAge of Revolutions: Progress and Backlash from 1600 to the PresentРейтинг: 4.5 из 5 звезд4.5/5 (9)
- Prisoners of Geography: Ten Maps That Explain Everything About the WorldОт EverandPrisoners of Geography: Ten Maps That Explain Everything About the WorldРейтинг: 4.5 из 5 звезд4.5/5 (1147)
- This Will Be My Undoing: Living at the Intersection of Black, Female, and Feminist in (White) AmericaОт EverandThis Will Be My Undoing: Living at the Intersection of Black, Female, and Feminist in (White) AmericaРейтинг: 4 из 5 звезд4/5 (78)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisОт EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (9)
- 1177 B.C.: The Year Civilization Collapsed: Revised and UpdatedОт Everand1177 B.C.: The Year Civilization Collapsed: Revised and UpdatedРейтинг: 4.5 из 5 звезд4.5/5 (111)
- His Needs, Her Needs: Building a Marriage That LastsОт EverandHis Needs, Her Needs: Building a Marriage That LastsРейтинг: 4.5 из 5 звезд4.5/5 (100)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4.5 из 5 звезд4.5/5 (6)
- Selling the Dream: The Billion-Dollar Industry Bankrupting AmericansОт EverandSelling the Dream: The Billion-Dollar Industry Bankrupting AmericansРейтинг: 4 из 5 звезд4/5 (19)
- The Wicked and the Willing: An F/F Gothic Horror Vampire NovelОт EverandThe Wicked and the Willing: An F/F Gothic Horror Vampire NovelРейтинг: 4 из 5 звезд4/5 (21)
- Our Little Secret: The True Story of a Teenage Killer and the Silence of a Small New England TownОт EverandOur Little Secret: The True Story of a Teenage Killer and the Silence of a Small New England TownРейтинг: 4.5 из 5 звезд4.5/5 (86)
- The Other Significant Others: Reimagining Life with Friendship at the CenterОт EverandThe Other Significant Others: Reimagining Life with Friendship at the CenterРейтинг: 4.5 из 5 звезд4.5/5 (2)
- When Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfОт EverandWhen Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfРейтинг: 5 из 5 звезд5/5 (36)
- Troubled: A Memoir of Foster Care, Family, and Social ClassОт EverandTroubled: A Memoir of Foster Care, Family, and Social ClassРейтинг: 4.5 из 5 звезд4.5/5 (27)
- American Jezebel: The Uncommon Life of Anne Hutchinson, the Woman Who Defied the PuritansОт EverandAmerican Jezebel: The Uncommon Life of Anne Hutchinson, the Woman Who Defied the PuritansРейтинг: 3.5 из 5 звезд3.5/5 (66)