Вам также может понравиться
- CAD - EBM September 2020 EditionДокумент17 страницCAD - EBM September 2020 EditionNaga Venkatamanoj Kumar PakalapatiОценок пока нет
- Bacillus Calmette - Guérin: Oral Polio VaccineДокумент1 страницаBacillus Calmette - Guérin: Oral Polio VaccineElleОценок пока нет
- Classification of Burns Based On Depth CharacteristicsДокумент2 страницыClassification of Burns Based On Depth CharacteristicsmexelleОценок пока нет
- Cardiac NSG DiagnosisДокумент5 страницCardiac NSG DiagnosisShreyas WalvekarОценок пока нет
- Case Presentation On Parkinson'S Disease: Presented By: T.Avinash Vith Pharm D Y13PHD0721Документ21 страницаCase Presentation On Parkinson'S Disease: Presented By: T.Avinash Vith Pharm D Y13PHD0721AVINASH TALAPALA100% (1)
- Transitional Care Case Study-Pulling It All TogetherДокумент13 страницTransitional Care Case Study-Pulling It All TogethermatthewОценок пока нет
- Nursing Case Study - With Final Slides.Документ77 страницNursing Case Study - With Final Slides.veejai_kumar100% (2)
- Lydia Hall: Reporters: Gwenn Marielle Galdo Kristine CustodioДокумент15 страницLydia Hall: Reporters: Gwenn Marielle Galdo Kristine CustodioKristine CustodioОценок пока нет
- DVT Case StudyДокумент2 страницыDVT Case StudyCrystal B Costa78Оценок пока нет
- HypertensionДокумент6 страницHypertensionTj Kevin P-DoctorОценок пока нет
- CasestudyutiДокумент21 страницаCasestudyutidael_05Оценок пока нет
- Assessment Diagnosis Inference Planning Intervention Rationale Outcomes Subjective DataДокумент2 страницыAssessment Diagnosis Inference Planning Intervention Rationale Outcomes Subjective DataJoan GuisicОценок пока нет
- Acute Care MapДокумент11 страницAcute Care Mapapi-301727553Оценок пока нет
- Demo Teaching Physical Health AssessmentДокумент5 страницDemo Teaching Physical Health AssessmentJulie May SuganobОценок пока нет
- Perioperative Nursing ManagementДокумент19 страницPerioperative Nursing ManagementSarah SeverreОценок пока нет
- Abnormal Midwifery: by Gladys M. BSN, KRCHNДокумент352 страницыAbnormal Midwifery: by Gladys M. BSN, KRCHNMercy KeruboОценок пока нет
- Airway ManagementДокумент63 страницыAirway ManagementGilang GumilangОценок пока нет
- Progress NoteДокумент3 страницыProgress NoteHaji JawaroОценок пока нет
- VSim Pharm (Mary Richards)Документ3 страницыVSim Pharm (Mary Richards)Jay Blastic's arts and FunОценок пока нет
- Pleural EffusionДокумент2 страницыPleural EffusionGellie Santos100% (1)
- Preeclampsia Case Presentation at 36 WeeksДокумент9 страницPreeclampsia Case Presentation at 36 WeeksSadiasifatafroz SifatОценок пока нет
- PATIENT 1 Nursing Assessment FormДокумент5 страницPATIENT 1 Nursing Assessment FormndemboloveОценок пока нет
- Al-Zaytoonah University ER Nursing LogДокумент5 страницAl-Zaytoonah University ER Nursing LogTahani KhalilОценок пока нет
- Week 5 CareplanДокумент2 страницыWeek 5 CareplanRaenell Curry100% (1)
- Discharge Summary PDFДокумент2 страницыDischarge Summary PDFbalab2311Оценок пока нет
- Essential Guide to Cerebral PalsyДокумент36 страницEssential Guide to Cerebral PalsyLeigh Ann Prosyne LozadaОценок пока нет
- Physical Assessment FindingsДокумент22 страницыPhysical Assessment FindingsKate CorderoОценок пока нет
- Med Surg MidtermДокумент17 страницMed Surg Midtermjhan grabierОценок пока нет
- Electrolyte ImbalanceДокумент4 страницыElectrolyte ImbalanceDoneva Lyn MedinaОценок пока нет
- West Visayas State University: Nursing ProcessДокумент4 страницыWest Visayas State University: Nursing ProcessPhylum Chordata100% (1)
- Care Planning for BreathlessnessДокумент14 страницCare Planning for BreathlessnesspriscellaОценок пока нет
- CACCN Certification Study Guide Questions Mar 2010Документ27 страницCACCN Certification Study Guide Questions Mar 2010BrittBrattDubb100% (1)
- VSim SARAH LIN For Nursing - Health Assessment POST QUIZДокумент5 страницVSim SARAH LIN For Nursing - Health Assessment POST QUIZWen RodsaОценок пока нет
- Anaesthesia For Patients With COPD: University College of Medical Sciences & GTB Hospital, DelhiДокумент76 страницAnaesthesia For Patients With COPD: University College of Medical Sciences & GTB Hospital, DelhiRINI100% (1)
- ChickenpoxДокумент2 страницыChickenpoxNorhana LangiОценок пока нет
- ST ND RDДокумент12 страницST ND RDwaterbuglilyОценок пока нет
- Ptl/Pprom and Multifetal Gestation: Anna Buabbud MD Ms3 LectureДокумент38 страницPtl/Pprom and Multifetal Gestation: Anna Buabbud MD Ms3 LectureNik C0% (1)
- Assignmen 1 AnswersДокумент3 страницыAssignmen 1 AnswersAlasl BobyОценок пока нет
- Oxytocic & TocolyticДокумент12 страницOxytocic & TocolyticFahmi Dwika Hafiz TrionoОценок пока нет
- Persuasive Communication in NursingДокумент4 страницыPersuasive Communication in NursingNicole Audrey JoaquinОценок пока нет
- Rheumatic FeverДокумент3 страницыRheumatic FeverPanji SaksonoОценок пока нет
- Review of Systems ANDREAДокумент7 страницReview of Systems ANDREAAndrea Dora OrtalizОценок пока нет
- Adults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofДокумент2 страницыAdults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofAlexandros MegasОценок пока нет
- Heat Stroke PatophysiologyДокумент48 страницHeat Stroke PatophysiologyMbenk NjoeОценок пока нет
- BS CareplanДокумент11 страницBS CareplanJulia BrownОценок пока нет
- Asthma: Chronic Inflammatory Airway DiseaseДокумент22 страницыAsthma: Chronic Inflammatory Airway DiseaseAnna EmОценок пока нет
- Initial Burn Assessment and CareДокумент39 страницInitial Burn Assessment and CareMudassir Mahboob KhattakОценок пока нет
- Transient Tachypnea of NewbornsДокумент16 страницTransient Tachypnea of NewbornsSelena Marie0% (1)
- Arc Guideline 11 1 Introduction To and Principles of in Hospital Resuscitation Feb 2019Документ22 страницыArc Guideline 11 1 Introduction To and Principles of in Hospital Resuscitation Feb 2019hernandez2812Оценок пока нет
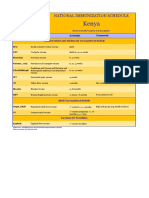
- Kenya Immunization ScheduleДокумент1 страницаKenya Immunization ScheduleDani AnyikaОценок пока нет
- COPD Case Presentation 1Документ19 страницCOPD Case Presentation 1Praveena Mogan100% (1)
- Woman With DysuriaДокумент26 страницWoman With DysuriaAlFi KamaliaОценок пока нет
- Intrauterine Growth RestrictionДокумент8 страницIntrauterine Growth Restrictionmalgosia7Оценок пока нет
- ThyroidectomyДокумент17 страницThyroidectomyDaryl Joshua SaturnoОценок пока нет
- Pulmonology Case Presentation on COPD ExacerbationДокумент20 страницPulmonology Case Presentation on COPD ExacerbationMohamad HafyfyОценок пока нет
- Medication ErrorДокумент3 страницыMedication Errortonlorenzcajipo100% (1)
- CCHIT Certified 2011 Ambulatory EHR Test Script 20100326Документ121 страницаCCHIT Certified 2011 Ambulatory EHR Test Script 20100326Zeeshan Ahmed KhanОценок пока нет
- HISTORY TAKING - FINAL - Sumanyu258@gmail - Com - 01092014 PDFДокумент111 страницHISTORY TAKING - FINAL - Sumanyu258@gmail - Com - 01092014 PDFRashmi RanjanОценок пока нет
- Labor and Delivery 34: Removing OvariesДокумент3 страницыLabor and Delivery 34: Removing OvariesDianneОценок пока нет
- Hyperbaric Oxygen Therapy For A Pediatric Electrical BurnДокумент3 страницыHyperbaric Oxygen Therapy For A Pediatric Electrical Burnsarah iriamanaОценок пока нет
- How acupuncture points modulate autonomic functionДокумент2 страницыHow acupuncture points modulate autonomic functionTrung Hiệp ĐàoОценок пока нет
- EE MOCK Test 2 Jan 2017 Questions OnlyДокумент28 страницEE MOCK Test 2 Jan 2017 Questions OnlyEmadSamirОценок пока нет
- Tugas Terjemahan-Manajemen NyeriДокумент50 страницTugas Terjemahan-Manajemen NyeriNur MuawanaОценок пока нет
- DrugsДокумент1 страницаDrugsMarnelie Guerrero AbuanОценок пока нет
- Nurs 501 Public Health Nursing IДокумент140 страницNurs 501 Public Health Nursing Iprincesssilver419Оценок пока нет
- 10 Healthiest Fermented FoodsДокумент5 страниц10 Healthiest Fermented FoodsbateriameaОценок пока нет
- HippocratesДокумент11 страницHippocratesalifОценок пока нет
- Health Optimizing Physical Education 1: 2 QuarterДокумент10 страницHealth Optimizing Physical Education 1: 2 QuarterAila Micaela KohОценок пока нет
- Definition-Acute Kidney InjuryДокумент6 страницDefinition-Acute Kidney Injuryashi leginОценок пока нет
- Ecology The Economy of Nature 7th Edition Ricklefs Test Bank DownloadДокумент19 страницEcology The Economy of Nature 7th Edition Ricklefs Test Bank DownloadApril Roberts100% (22)
- Sex Linked Practice Problems TCДокумент17 страницSex Linked Practice Problems TCanon_11091143Оценок пока нет
- Course Syllabus: Course Code Course Title ECTS CreditsДокумент3 страницыCourse Syllabus: Course Code Course Title ECTS CreditsHanaa HamadallahОценок пока нет
- PDF Dis StandardsДокумент35 страницPDF Dis StandardsEdén PastoraОценок пока нет
- GE Trees Threaten Forests and BiodiversityДокумент14 страницGE Trees Threaten Forests and BiodiversityIvica KelamОценок пока нет
- Fermented BiocharДокумент81 страницаFermented Biocharstar662100% (1)
- When I hear the noiseДокумент2 страницыWhen I hear the noiseh00nguy0n-18Оценок пока нет
- NGT FeedingДокумент2 страницыNGT FeedingValones BeaОценок пока нет
- The Insulin Receptor and Mechanism of ActionДокумент5 страницThe Insulin Receptor and Mechanism of ActionMonica AbabeiОценок пока нет
- Endocrine Disorders and PregnancyДокумент32 страницыEndocrine Disorders and PregnancyChristine Marie BudlaoОценок пока нет
- Chelating Therapy: Azeem ImamДокумент14 страницChelating Therapy: Azeem Imamazeem imamОценок пока нет
- 66Документ82 страницы66Ankit kumar singhОценок пока нет
- Advances in The Treatment of Sickle CellДокумент15 страницAdvances in The Treatment of Sickle CellMayuri P KОценок пока нет
- Feeling BlueДокумент2 страницыFeeling BlueSAKHAWAT HOSSAIN KHAN MDОценок пока нет
- LRD DIV SPE FM 001a RITM Lab Test Request Form - Clinical Lab 1Документ1 страницаLRD DIV SPE FM 001a RITM Lab Test Request Form - Clinical Lab 1Megen PLCОценок пока нет
- Facial NerveДокумент128 страницFacial NervevaneetОценок пока нет
- Essential Principles of Primary Health CareДокумент25 страницEssential Principles of Primary Health CareEmily BernatОценок пока нет
- Top Communicable Diseases in The Philippines 2019Документ4 страницыTop Communicable Diseases in The Philippines 2019Nicole cuencosОценок пока нет
- 2010 SPN BL Rez MALDI TOFДокумент12 страниц2010 SPN BL Rez MALDI TOFSergey SidorenkoОценок пока нет
- Esophageal Cancer NewДокумент52 страницыEsophageal Cancer Newapi-282115150Оценок пока нет