Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Prevalence of Autism Spectrum Disorders in A Total Population Sample in A South Korean Community - 2011Документ9 страницPrevalence of Autism Spectrum Disorders in A Total Population Sample in A South Korean Community - 2011info-TEAОценок пока нет
- Annual Research Review - Re-Thinking The Classification of Autism Spectrum Disorders-2Документ20 страницAnnual Research Review - Re-Thinking The Classification of Autism Spectrum Disorders-2info-TEAОценок пока нет
- AUTISM in BRAZIL - Perspectives From Science and Society - Paula Cristiane - Erik Fombonne 2011Документ4 страницыAUTISM in BRAZIL - Perspectives From Science and Society - Paula Cristiane - Erik Fombonne 2011info-TEAОценок пока нет
- Some Elements About The Prevalence of Autism Spectrum Disorders (ASD) in The European Union (2005)Документ16 страницSome Elements About The Prevalence of Autism Spectrum Disorders (ASD) in The European Union (2005)info-TEAОценок пока нет
- Prevalence and Services in Countries Outside of Europe and North AmericaДокумент40 страницPrevalence and Services in Countries Outside of Europe and North Americalorenzofranchi6371Оценок пока нет
- The Worldwide Prevalence of ADHD (Attention-Deficit/hyperactivity Disorder) : Is It An American Condition?Документ10 страницThe Worldwide Prevalence of ADHD (Attention-Deficit/hyperactivity Disorder) : Is It An American Condition?info-TEAОценок пока нет
- Es El Pronostico A Largo Plazo de TGD-NE Diferente Del de Trastorno Autista?-En Inglés. 2011, NoruegaДокумент9 страницEs El Pronostico A Largo Plazo de TGD-NE Diferente Del de Trastorno Autista?-En Inglés. 2011, Noruegainfo-TEAОценок пока нет
- TDAH, Trastorno Por Déficit de Atención Con Hiperactividad en Adultos: Caracterización Clínica y TerapéuticaДокумент7 страницTDAH, Trastorno Por Déficit de Atención Con Hiperactividad en Adultos: Caracterización Clínica y Terapéuticainfo-TEA50% (2)
- Tratamineto Farmacologico Del Retraso Mental - Artigas - Articulo PDFДокумент7 страницTratamineto Farmacologico Del Retraso Mental - Artigas - Articulo PDFGabriel Basurto MaciasОценок пока нет
- Dificultades en Evaluación y Diagnóstico Del Autismo. Una Discusión - México - 2008Документ8 страницDificultades en Evaluación y Diagnóstico Del Autismo. Una Discusión - México - 2008info-TEAОценок пока нет
- Ultimo Reporte de Prevalencia de TEA (EE - UU.)Документ51 страницаUltimo Reporte de Prevalencia de TEA (EE - UU.)info-TEAОценок пока нет
- Trastorno Oposicionista DesafianteДокумент6 страницTrastorno Oposicionista DesafiantesandrixmbОценок пока нет
- CDC Autism Study, March 2012Документ24 страницыCDC Autism Study, March 2012The Salt Lake TribuneОценок пока нет
- Condiciones Tempranas Del Desarrollo y El Aprendizaje: El Papel de Las Funciones EjecutivasДокумент9 страницCondiciones Tempranas Del Desarrollo y El Aprendizaje: El Papel de Las Funciones Ejecutivasinfo-TEAОценок пока нет
- Atención Temprana de Las Dificultades de AprendizajeДокумент4 страницыAtención Temprana de Las Dificultades de Aprendizajeinfo-TEA100% (1)
- Desarrollo Temprano, Autismo y Trastornos Del Lenguaje (J.Martos)Документ8 страницDesarrollo Temprano, Autismo y Trastornos Del Lenguaje (J.Martos)info-TEAОценок пока нет
- Autismo y X FragilДокумент4 страницыAutismo y X FragilCamila Belen Vega GonzalezОценок пока нет
- Autism Europe, PERSONS WITH AUTISM SPECTRUM DISORDERS Identification, Understanding, InterventionДокумент28 страницAutism Europe, PERSONS WITH AUTISM SPECTRUM DISORDERS Identification, Understanding, Interventioninfo-TEAОценок пока нет
- Early Regression in Social Communication in Autism Spectrum Disorders: A CPEA Study (Luyster Et Al 2005)Документ26 страницEarly Regression in Social Communication in Autism Spectrum Disorders: A CPEA Study (Luyster Et Al 2005)info-TEAОценок пока нет
- Nueva Zelanda Asd Guideline Summary Apr 2008 (En Inglés)Документ26 страницNueva Zelanda Asd Guideline Summary Apr 2008 (En Inglés)info-TEAОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Foley-Nicpon 2017Документ13 страницFoley-Nicpon 2017Jennifer TanОценок пока нет
- Kanne Gerber Et Al Vineland 2010Документ12 страницKanne Gerber Et Al Vineland 2010Gh8jfyjnОценок пока нет
- Brief Observation of Symptoms of Autism - Version 7-28-20Документ48 страницBrief Observation of Symptoms of Autism - Version 7-28-20Macarena Ignacia Argaluza Guerrero100% (3)
- Strange Stories Happe 2009Документ22 страницыStrange Stories Happe 2009Arturo GaytánОценок пока нет
- Autism Spectrum Disorders Foundations Characteristics and Effective Strategies 2nd Edition Ebook PDF VersionДокумент58 страницAutism Spectrum Disorders Foundations Characteristics and Effective Strategies 2nd Edition Ebook PDF Versionmatthew.grasso983100% (42)
- SOS Test Psixometrika SosДокумент120 страницSOS Test Psixometrika SosAlexis PsaroudakisОценок пока нет
- DiscoДокумент19 страницDiscovcuadrosvОценок пока нет
- Son Rise PDFДокумент12 страницSon Rise PDFMaximMadalinaIulianaОценок пока нет
- Robertson 1999Документ8 страницRobertson 1999Wanessa AndradeОценок пока нет
- Characterization of Special Interests in Autism Spectrum Disorder Special Interests SurveyДокумент15 страницCharacterization of Special Interests in Autism Spectrum Disorder Special Interests SurveyValpe PsicólogosОценок пока нет
- Social Communication Questionnaire (SCQ)Документ4 страницыSocial Communication Questionnaire (SCQ)Wade WilsonОценок пока нет
- Research in Autism Spectrum Disorders: Sylvie GoldmanДокумент5 страницResearch in Autism Spectrum Disorders: Sylvie GoldmanMilo Due100% (1)
- 1 - Aripiprazole in The Treatment 52 Minggu AutismДокумент8 страниц1 - Aripiprazole in The Treatment 52 Minggu AutismmirafauziОценок пока нет
- A Pilot Study On The Effects of Orff-Based Therapeutic Music in Children With Autism Spectrum DisorderДокумент9 страницA Pilot Study On The Effects of Orff-Based Therapeutic Music in Children With Autism Spectrum DisorderSushma KaushikОценок пока нет
- Clinical Assessment of Child and Adolescent Personality and Behavior (Fourth Edition)Документ21 страницаClinical Assessment of Child and Adolescent Personality and Behavior (Fourth Edition)Sam Ficher0% (2)
- Lai M-C, Lombardo MV, Ruigrok ANV, Chakrabarti B, Auyeung B, Szatmari P, Et Al. (2017) - Quantifying and Exploring Camouflaging in Men and WomenДокумент13 страницLai M-C, Lombardo MV, Ruigrok ANV, Chakrabarti B, Auyeung B, Szatmari P, Et Al. (2017) - Quantifying and Exploring Camouflaging in Men and WomenTomislav CvrtnjakОценок пока нет
- Autism Spectrum DisorderДокумент25 страницAutism Spectrum DisorderDrSk Samim100% (1)
- Journal Pre-Proof: Seminars in Pediatric NeurologyДокумент43 страницыJournal Pre-Proof: Seminars in Pediatric NeurologyDaniele PendezaОценок пока нет
- ASD DSM-5 Parent Interview FinalДокумент10 страницASD DSM-5 Parent Interview FinaltammyОценок пока нет
- Fractionating Autism Based On Neuroanatomical Normative ModelingДокумент10 страницFractionating Autism Based On Neuroanatomical Normative ModelingTaNiTa TiKaRaNОценок пока нет
- BOSA Example Clinical SummariesДокумент5 страницBOSA Example Clinical SummariesMacarena Ignacia Argaluza Guerrero100% (3)
- New Research: Patricia Howlin,, Philippa Moss,, Sarah Savage,, Michael RutterДокумент11 страницNew Research: Patricia Howlin,, Philippa Moss,, Sarah Savage,, Michael RutterTomislav CvrtnjakОценок пока нет
- Autism Diagnostic Observation Schedule - Second Edition (ADOS-2)Документ5 страницAutism Diagnostic Observation Schedule - Second Edition (ADOS-2)shizuka samaОценок пока нет
- Bedford Et Al-2016-Autism ResearchДокумент9 страницBedford Et Al-2016-Autism ResearchRosa Fonseca AguloОценок пока нет
- 2019 - Changing Conceptualizations of Regression in Autism - OzonoffДокумент9 страниц2019 - Changing Conceptualizations of Regression in Autism - OzonoffJesus RiveraОценок пока нет
- Promoting Child-Initiated Social-Communication in Children With Autism: Son-Rise Program Intervention EffectsДокумент13 страницPromoting Child-Initiated Social-Communication in Children With Autism: Son-Rise Program Intervention EffectsErik NuminenОценок пока нет
- Baremos Faux PassДокумент20 страницBaremos Faux PassMaria Clara RonquiОценок пока нет
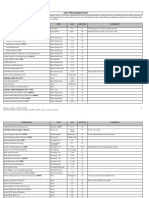
- List of Psychological TestsДокумент15 страницList of Psychological Testsnauw zОценок пока нет
- 1 Clinical Assessments Catalogue 2016 Autism Spectrum DisordersДокумент20 страниц1 Clinical Assessments Catalogue 2016 Autism Spectrum Disorderszubaida sharifОценок пока нет
- Grodberg Et Al., 2015 Diagnostico Observacional Simplificado en AutismoДокумент7 страницGrodberg Et Al., 2015 Diagnostico Observacional Simplificado en AutismoRicardo Jose De LeonОценок пока нет