Вам также может понравиться
- Short ImplantsОт EverandShort ImplantsBoyd J. TomasettiОценок пока нет
- Crack Tooth (ADJ)Документ6 страницCrack Tooth (ADJ)Kasturi SriramОценок пока нет
- Ferrule EffectДокумент11 страницFerrule EffectJaysondeAsisОценок пока нет
- Kurtzman Restoration of Endodontically Treated TeethДокумент8 страницKurtzman Restoration of Endodontically Treated TeethAdelia CaryabudiОценок пока нет
- NBDE Remembered 2 New YorkДокумент242 страницыNBDE Remembered 2 New YorkR MОценок пока нет
- Criteria For Restorable Endo Teetg - CDA-ADC JournalДокумент9 страницCriteria For Restorable Endo Teetg - CDA-ADC Journalmoji_puiОценок пока нет
- Management Flabby RidgeДокумент4 страницыManagement Flabby RidgeNidya Patricia Sembiring100% (1)
- Practice: Orthodontics. Part 9: Anchorage Control and Distal MovementДокумент9 страницPractice: Orthodontics. Part 9: Anchorage Control and Distal MovementAnonymous ENwjWryОценок пока нет
- Reduction Resto ProcedureДокумент5 страницReduction Resto ProcedureAnindyaNoviaPutriОценок пока нет
- Occlusal Change Through Orthodontics in TMD Patients: Issue Date: October 2007, Posted On: 11/1/2007Документ4 страницыOcclusal Change Through Orthodontics in TMD Patients: Issue Date: October 2007, Posted On: 11/1/2007smritiОценок пока нет
- Space LossДокумент5 страницSpace LossAsma NawazОценок пока нет
- What Is The Diagnose?: Source: 2Документ7 страницWhat Is The Diagnose?: Source: 2Reischa Tiara HardiyaniОценок пока нет
- Single Complete Denture FinalДокумент15 страницSingle Complete Denture FinalVikas AggarwalОценок пока нет
- Mobility and Biological Rationale For Splinting Teeth: Tooth TheДокумент8 страницMobility and Biological Rationale For Splinting Teeth: Tooth TheJamaludin NawawiОценок пока нет
- Content ServerДокумент4 страницыContent ServerJose Antonio Figuroa AbadoОценок пока нет
- Kokich CaninosДокумент6 страницKokich CaninosMercedes RojasОценок пока нет
- Prepared Cavities On The StrenДокумент4 страницыPrepared Cavities On The StrenPriyank RaiОценок пока нет
- Management of Cracked Tooth Syndrome A C PDFДокумент6 страницManagement of Cracked Tooth Syndrome A C PDFElizabeth CortésОценок пока нет
- 2007 - Intrusion of Overerupted Molars byДокумент7 страниц2007 - Intrusion of Overerupted Molars byTien Li AnОценок пока нет
- Fracture Resistant Endodontic and Restorative PreparationsДокумент11 страницFracture Resistant Endodontic and Restorative PreparationsCassiano CapellassiОценок пока нет
- Maheaswari CL PDFДокумент5 страницMaheaswari CL PDFdorasani99Оценок пока нет
- Fixed Removable ProstheTicsДокумент9 страницFixed Removable ProstheTicsSumi AliОценок пока нет
- Types of SplintsДокумент9 страницTypes of SplintsRatri ReswitadewiОценок пока нет
- Literature ReviewДокумент3 страницыLiterature ReviewPuteri NazirahОценок пока нет
- Cuspal Flexure and Stress in Restored Teeth Caused by Amalgam ExpansionДокумент8 страницCuspal Flexure and Stress in Restored Teeth Caused by Amalgam ExpansionPablo BenitezОценок пока нет
- Forced Eruption of Adjoining Maxillary Premolars Using A Removable Orthodontic Appliance: A Case ReportДокумент4 страницыForced Eruption of Adjoining Maxillary Premolars Using A Removable Orthodontic Appliance: A Case Reportikeuchi_ogawaОценок пока нет
- Biomechanical Considerations in Restoring Endodontically Treated Teeth-Assif1994Документ3 страницыBiomechanical Considerations in Restoring Endodontically Treated Teeth-Assif1994Dan MPОценок пока нет
- Interesting Eruption of 4 Teeth Associated With A Large Dentigerous Cyst in Mandible by Only MarsupializationДокумент3 страницыInteresting Eruption of 4 Teeth Associated With A Large Dentigerous Cyst in Mandible by Only MarsupializationAnupama NagrajОценок пока нет
- Restoration of Esthetics And.... POST COREДокумент6 страницRestoration of Esthetics And.... POST COREnadeemОценок пока нет
- SD-V9N1 Bosshart CompleteДокумент7 страницSD-V9N1 Bosshart CompleteAnonymous gjrAZMXB3Оценок пока нет
- 08-Implant Surgery PDFДокумент15 страниц08-Implant Surgery PDFalkhalijia dentalОценок пока нет
- Gutiera de BruxismДокумент3 страницыGutiera de BruxismAlin AniculaesaОценок пока нет
- COSMETIC DENTISTRY: The Full Mouth Fixed Rehabilitation of The Bruxing Patient - Achieving Function and EstheticsДокумент7 страницCOSMETIC DENTISTRY: The Full Mouth Fixed Rehabilitation of The Bruxing Patient - Achieving Function and EstheticsPrima Agung LОценок пока нет
- Extractions in OrthodonticsДокумент6 страницExtractions in OrthodonticsZubair AhmedОценок пока нет
- Immediate Temporization Crown Lengthening: April 2011 Volume 32, Issue 3Документ6 страницImmediate Temporization Crown Lengthening: April 2011 Volume 32, Issue 3Kyoko C.LОценок пока нет
- Biomechanics of Post Core SystemДокумент18 страницBiomechanics of Post Core SystemNourhan IbrahimОценок пока нет
- Tooth Fracture in Vivo and in VitroДокумент9 страницTooth Fracture in Vivo and in VitroTing-han LinОценок пока нет
- 2016 Salvation of Severely Fractured Anterior Tooth An Orthodontic ApproachДокумент4 страницы2016 Salvation of Severely Fractured Anterior Tooth An Orthodontic ApproachRajesh GyawaliОценок пока нет
- The Effects of Splinting Periodontally Compromised Removable Partial Denture Abutments On Bone Stresses: A Three-Dimensional Finite Element StudyДокумент7 страницThe Effects of Splinting Periodontally Compromised Removable Partial Denture Abutments On Bone Stresses: A Three-Dimensional Finite Element StudytovarichОценок пока нет
- Ferrule Effect DiscussionДокумент4 страницыFerrule Effect DiscussionBinu P NairОценок пока нет
- Slow Maxillary Expansion A Review 209085c4Документ12 страницSlow Maxillary Expansion A Review 209085c4jabbarОценок пока нет
- Pin-Retained Restoration With Resin Bonded Composite of A Badly Broken ToothДокумент3 страницыPin-Retained Restoration With Resin Bonded Composite of A Badly Broken ToothIOSRjournalОценок пока нет
- 8 - Maxillary Expansion in Nongrowing Patients. Conventional, SurgicalДокумент11 страниц8 - Maxillary Expansion in Nongrowing Patients. Conventional, SurgicalMariana SantosОценок пока нет
- Trauma From OcclusionДокумент3 страницыTrauma From OcclusionSuganya MurugaiahОценок пока нет
- s12903 018 0549 8Документ7 страницs12903 018 0549 8JeanpareОценок пока нет
- Endodontic Management of Traumatic InjuriesДокумент6 страницEndodontic Management of Traumatic InjuriesMehwish MunawarОценок пока нет
- Traction-A Swgical /orthodontic Procedure: L. J. Mcbride, L.D.S., R.C.S., D. OrthДокумент13 страницTraction-A Swgical /orthodontic Procedure: L. J. Mcbride, L.D.S., R.C.S., D. OrthMarcos CastroОценок пока нет
- Shortened Dental ArchДокумент5 страницShortened Dental Archsarah wilderОценок пока нет
- Single Complete DentureДокумент12 страницSingle Complete DentureHarsha Reddy100% (1)
- Mancebo Effect of Tooh Type and Ferrule On The SurvivalДокумент6 страницMancebo Effect of Tooh Type and Ferrule On The SurvivalagusaranpОценок пока нет
- 3 Single CDДокумент7 страниц3 Single CDdrgayen6042Оценок пока нет
- Mel Sen 1994Документ12 страницMel Sen 1994Lynda M. NaranjoОценок пока нет
- Emdogain 1Документ6 страницEmdogain 1Nicco MarantsonОценок пока нет
- Stress Distribution in Molars Restored With Inlays or Onlays With or Without Endodontic Treatment: A Three-Dimensional Finite Element AnalysisДокумент7 страницStress Distribution in Molars Restored With Inlays or Onlays With or Without Endodontic Treatment: A Three-Dimensional Finite Element AnalysismusaabsiddiquiОценок пока нет
- The Size of Occlusal Rest Seats PreparedДокумент7 страницThe Size of Occlusal Rest Seats PreparedPatra PrimadanaОценок пока нет
- Dentigerous Cyst Associated With Permanent Maxillary Central Incisor: Report of Two CasesДокумент4 страницыDentigerous Cyst Associated With Permanent Maxillary Central Incisor: Report of Two CasesAhmad MustafaОценок пока нет
- 3501029Документ5 страниц3501029Anil NepalОценок пока нет
- Article1404395371 - Shibu and RajanДокумент3 страницыArticle1404395371 - Shibu and RajanRuchi ShahОценок пока нет
- Application Form Screening Exam 2009Документ15 страницApplication Form Screening Exam 2009Maheswari SureshОценок пока нет
- Dci Screening Test GazetteДокумент11 страницDci Screening Test GazetteMaheswari SureshОценок пока нет
- Mechanical Properties of Wires and Its Orthodontic ApplicationДокумент12 страницMechanical Properties of Wires and Its Orthodontic Applicationabhishek_meenuОценок пока нет
- C++: Object-Oriented ProgrammingДокумент31 страницаC++: Object-Oriented ProgrammingMaheswari SureshОценок пока нет
- OopsДокумент1 страницаOopsMaheswari SureshОценок пока нет
- Cracked Tooth SyndromeДокумент6 страницCracked Tooth SyndromeFar NazОценок пока нет
- New - BMP3005 - ABF - Assessment Brief - FДокумент5 страницNew - BMP3005 - ABF - Assessment Brief - Fmilka traykovОценок пока нет
- Micronet TMRДокумент316 страницMicronet TMRHaithem BrebishОценок пока нет
- NSTP SlabДокумент2 страницыNSTP SlabCherine Fates MangulabnanОценок пока нет
- Knitting in Satellite AntennaДокумент4 страницыKnitting in Satellite AntennaBhaswati PandaОценок пока нет
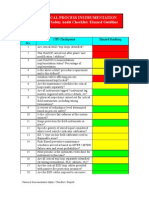
- Chemical Safety ChecklistДокумент3 страницыChemical Safety ChecklistPillai Sreejith100% (10)
- Caldon Lefm 240ci Ultrasonic Flow Meters: Integral Manifold DesignДокумент6 страницCaldon Lefm 240ci Ultrasonic Flow Meters: Integral Manifold DesignJim LimОценок пока нет
- Forensic My Cology Mcgraw HillДокумент8 страницForensic My Cology Mcgraw HillJayanti RaufОценок пока нет
- Pell (2017) - Trends in Real-Time Traffic SimulationДокумент8 страницPell (2017) - Trends in Real-Time Traffic SimulationJorge OchoaОценок пока нет
- ENG 102 Essay PromptДокумент2 страницыENG 102 Essay Promptarshia winОценок пока нет
- D15 Hybrid P1 QPДокумент6 страницD15 Hybrid P1 QPShaameswary AnnadoraiОценок пока нет
- Heisenberg, "Über Den Anschaulichen Inhalt Der Quantentheoretischen Kinematik Und Mechanik"Документ16 страницHeisenberg, "Über Den Anschaulichen Inhalt Der Quantentheoretischen Kinematik Und Mechanik"Benjamin Crowell0% (1)
- B2B Marketing: Chapter-8Документ23 страницыB2B Marketing: Chapter-8Saurabh JainОценок пока нет
- Demand Determinants EEMДокумент22 страницыDemand Determinants EEMPrabha KaranОценок пока нет
- Wind Turbines - I. Al-BahadlyДокумент664 страницыWind Turbines - I. Al-Bahadlykevin_leigh_1Оценок пока нет
- Accounting System (Compatibility Mode) PDFДокумент10 страницAccounting System (Compatibility Mode) PDFAftab AlamОценок пока нет
- Introduction To Pharmacology by ZebДокумент31 страницаIntroduction To Pharmacology by ZebSanam MalikОценок пока нет
- Template Remarks For IIДокумент18 страницTemplate Remarks For IIjasleeneceОценок пока нет
- Datalogic tl46 A Manual - 230104 - 140343Документ2 страницыDatalogic tl46 A Manual - 230104 - 140343Emmanuel Baldenegro PadillaОценок пока нет
- Straw Bale ConstructionДокумент37 страницStraw Bale ConstructionelissiumОценок пока нет
- Firing OrderДокумент5 страницFiring OrderCurtler PaquibotОценок пока нет
- Hansen Aise Im Ch12Документ66 страницHansen Aise Im Ch12Rizki19maretОценок пока нет
- Reservoir Bag Physics J PhilipДокумент44 страницыReservoir Bag Physics J PhilipJashim JumliОценок пока нет
- Acute Leukemia The Scientist's Perspective and ChallengeДокумент438 страницAcute Leukemia The Scientist's Perspective and ChallengemedskyqqОценок пока нет
- Corporate Valuation WhartonДокумент6 страницCorporate Valuation Whartonebrahimnejad64Оценок пока нет
- IBS and SIBO Differential Diagnosis, SiebeckerДокумент1 страницаIBS and SIBO Differential Diagnosis, SiebeckerKrishna DasОценок пока нет
- Amsterdam Pipe Museum - Snuff WorldwideДокумент1 страницаAmsterdam Pipe Museum - Snuff Worldwideevon1Оценок пока нет
- Research Paper On Marketing PlanДокумент4 страницыResearch Paper On Marketing Planfvhacvjd100% (1)
- Thesis Topics in Medicine in Delhi UniversityДокумент8 страницThesis Topics in Medicine in Delhi UniversityBecky Goins100% (2)
- Corregidor Title DefenseДокумент16 страницCorregidor Title DefenseJaydee ColadillaОценок пока нет
- Blank FacebookДокумент2 страницыBlank Facebookapi-355481535Оценок пока нет