Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Chapter 6b Digital SurgeryДокумент18 страницChapter 6b Digital SurgerypodmmgfОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Chapter 4e Internal MedicineДокумент19 страницChapter 4e Internal MedicinepodmmgfОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Chapter 5 Pediatric PodiatryДокумент88 страницChapter 5 Pediatric Podiatrypodmmgf100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Chapter 4d Podiatric Infectious DiseasesДокумент20 страницChapter 4d Podiatric Infectious DiseasespodmmgfОценок пока нет
- Chapter 4 and 4a Introduction To Medicine and DermatologyДокумент16 страницChapter 4 and 4a Introduction To Medicine and DermatologypodmmgfОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Chapter 3g Physical MedicineДокумент20 страницChapter 3g Physical MedicinepodmmgfОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- PathoMechanics PDFДокумент36 страницPathoMechanics PDFMagnus SigaarssonОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Chapter 3e Pathological GaitДокумент8 страницChapter 3e Pathological GaitpodmmgfОценок пока нет
- Care of Clients With Physiologic and Psychosocial AlterationsДокумент34 страницыCare of Clients With Physiologic and Psychosocial AlterationsChloie Marie RosalejosОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Med Surg Respiratory SystemДокумент173 страницыMed Surg Respiratory Systembamfalcon100% (4)
- Session 3 Pathophysiology of COPD and AsthmaДокумент40 страницSession 3 Pathophysiology of COPD and AsthmaOsamaMazhariОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Pulm HTN WilcoxДокумент11 страницPulm HTN WilcoxyersiniapestismorОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- GINA 2017 Teaching Slide Set FullДокумент17 страницGINA 2017 Teaching Slide Set FullLorenzoVasquezDatul100% (3)
- NCP GunshotДокумент13 страницNCP GunshotMichael John F. Natividad0% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Formic Acid C BASF Medguidelines E036Документ4 страницыFormic Acid C BASF Medguidelines E036varrsinneОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Case Study For DiscussionДокумент3 страницыCase Study For DiscussionSiti nur Kholifatus samsiyahОценок пока нет
- Chapter 2 Respiratory AssessmentДокумент9 страницChapter 2 Respiratory AssessmentKathleen Dela CruzОценок пока нет
- Respiratory Distress Syndrome of The Newborn JCG0086 v3Документ17 страницRespiratory Distress Syndrome of The Newborn JCG0086 v3meutia salsabilaОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- An Essay On "Covid-19 Pandemic" by Prof. Dr. Mustafa Asim SafakДокумент9 страницAn Essay On "Covid-19 Pandemic" by Prof. Dr. Mustafa Asim Safakkasmakiprawi72Оценок пока нет
- NCP For BronchitisДокумент2 страницыNCP For BronchitisJefherrson Nericua Jemilo50% (2)
- Assessment Nursing Diagnosis Background Knowledge Planning Intervention Rationale Evaluation Subjective: Short Term: Independent: IndependentДокумент4 страницыAssessment Nursing Diagnosis Background Knowledge Planning Intervention Rationale Evaluation Subjective: Short Term: Independent: IndependentAlyssa Marie SantosОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- NURS FPX 6021 Assessment 1 Concept MapДокумент7 страницNURS FPX 6021 Assessment 1 Concept MapCarolyn HarkerОценок пока нет
- Gregori Graboboi - Quick Code ListДокумент20 страницGregori Graboboi - Quick Code Listondasdeforma93% (29)
- International Emergency NursingДокумент6 страницInternational Emergency NursingAtika AlfiaОценок пока нет
- Assessment Diagnosis Background Knowledge Plan of Care Nursing Intervention S Rationale EvaluationДокумент3 страницыAssessment Diagnosis Background Knowledge Plan of Care Nursing Intervention S Rationale Evaluationtin911Оценок пока нет
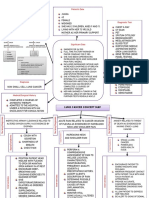
- Lung Cancer Concept Map-Group 2Документ2 страницыLung Cancer Concept Map-Group 2Maria Cristina100% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Anaphylaxis Clinical PresentationДокумент9 страницAnaphylaxis Clinical Presentationilhampaneja_x3Оценок пока нет
- The Thorax and Lungs - BATESДокумент4 страницыThe Thorax and Lungs - BATESsitalcoolk100% (2)
- CC-Concept Map 2Документ5 страницCC-Concept Map 2MDCITY50% (2)
- Reexpansion Pulmonary Edema : UpdateДокумент6 страницReexpansion Pulmonary Edema : UpdateWenny EudensiaОценок пока нет
- MCQ About Pulmonary-DiseaseДокумент31 страницаMCQ About Pulmonary-Diseaseمجتبى عليОценок пока нет
- Abdominal Aortic AneurysmДокумент10 страницAbdominal Aortic AneurysmPrince K. TaileyОценок пока нет
- RLE - Reviewer - OxygenationДокумент14 страницRLE - Reviewer - OxygenationVinzii DrtОценок пока нет
- HSNS264 Case StudyДокумент8 страницHSNS264 Case StudySophie AndersonОценок пока нет
- Clinical Manifestations and Assessment of Respiratory Disease 5th Edition Jardins Test BankДокумент36 страницClinical Manifestations and Assessment of Respiratory Disease 5th Edition Jardins Test Bankgeincupola.06zi100% (23)
- Antibiotics For Treatment and Prevention of Exacerbations of Chronic Obstructive Pulmonary DiseaseДокумент19 страницAntibiotics For Treatment and Prevention of Exacerbations of Chronic Obstructive Pulmonary DiseaseAvila CulenОценок пока нет
- Respiratory System: Study: Pulmonology Physician: Pulmonologist Function: Exchange of GasesДокумент5 страницRespiratory System: Study: Pulmonology Physician: Pulmonologist Function: Exchange of GasesSakshi BishnoiОценок пока нет
- BisinosisДокумент4 страницыBisinosisMaría IgnaciaОценок пока нет