Вам также может понравиться
- Cast and TractionДокумент7 страницCast and Tractionnamme01_margateОценок пока нет
- Orthopedic Casts ExplainedДокумент37 страницOrthopedic Casts ExplainedShiiza Dusong Tombucon-AsisОценок пока нет
- Cast and BandagesДокумент5 страницCast and BandagesNoey TabangcuraОценок пока нет
- Casts immobilize broken bones as they healДокумент30 страницCasts immobilize broken bones as they healKatrina PonceОценок пока нет
- Cast and MoldsДокумент11 страницCast and Moldskaliente0118Оценок пока нет
- 4-Conservative Treatment FX, CastingДокумент53 страницы4-Conservative Treatment FX, CastingMuhammad TaqwaОценок пока нет
- Ankle SprainДокумент4 страницыAnkle SprainLaurencia LenyОценок пока нет
- Cast CareДокумент4 страницыCast CareRogelyn PatriarcaОценок пока нет
- Cause: StatisticsДокумент6 страницCause: StatisticsKatherine Vergara ManejaОценок пока нет
- Tips for Everyday Life and Sports With an Artificial Joint: Expert guidebook for dealing with a prosthesis for patients with a new hip or knee jointОт EverandTips for Everyday Life and Sports With an Artificial Joint: Expert guidebook for dealing with a prosthesis for patients with a new hip or knee jointОценок пока нет
- CastДокумент7 страницCastRegina Nina YoshidaОценок пока нет
- What Is Lateral Collateral Ligament Sprain?Документ9 страницWhat Is Lateral Collateral Ligament Sprain?mochamad ilham kurniaОценок пока нет
- Patella TendonitisДокумент43 страницыPatella Tendonitisvijkris1985100% (2)
- Traction Two-1Документ20 страницTraction Two-1pascalmugodoОценок пока нет
- MSK Examination, Evaluation of Foot and Ankle DisordersДокумент8 страницMSK Examination, Evaluation of Foot and Ankle DisordersSharjeel AmjadОценок пока нет
- Trochanteric BursitisДокумент3 страницыTrochanteric BursitisCat Graverobber Iskariot100% (2)
- Understanding: Knowing The Culprit: The Gaming PostureДокумент8 страницUnderstanding: Knowing The Culprit: The Gaming Posturecrisanto valdezОценок пока нет
- Anatomy of The AnkleДокумент8 страницAnatomy of The Ankleallie343343Оценок пока нет
- Is The Use of A Pulling Force To Treat Muscle and Skeleton DisordersДокумент42 страницыIs The Use of A Pulling Force To Treat Muscle and Skeleton DisordersShane Arianne Faye BaldoveОценок пока нет
- The Musculoskeletal System...Документ24 страницыThe Musculoskeletal System...Charity Grace Magno67% (3)
- Foot AnkleДокумент11 страницFoot AnklelassieladdieОценок пока нет
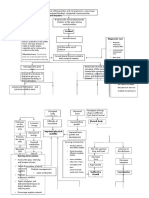
- Pathway - Skoliosis GROUPДокумент12 страницPathway - Skoliosis GROUPAnonymous NZTQVgjaОценок пока нет
- Rotator Cuff Repair EbookДокумент31 страницаRotator Cuff Repair EbookJohnPaulBascoОценок пока нет
- Internship Acknowledgement at Hospital Slim RiverДокумент28 страницInternship Acknowledgement at Hospital Slim RiverradicalmpОценок пока нет
- Rotator Cuff Tears Orthoinfo - Aaos.org TopicДокумент7 страницRotator Cuff Tears Orthoinfo - Aaos.org TopicMontserrat LandaОценок пока нет
- LilianДокумент5 страницLilianLilian Laureto SabinesОценок пока нет
- Ankle Sprain EbookДокумент19 страницAnkle Sprain EbookJohnPaulBascoОценок пока нет
- Walking CruthesДокумент15 страницWalking Cruthesanna Tanur100% (1)
- FRAKTURE CasesДокумент6 страницFRAKTURE CasesJM MARQUEZОценок пока нет
- Healthy Shoulder Handbook: 100 Exercises for Treating and Preventing Frozen Shoulder, Rotator Cuff and other Common InjuriesОт EverandHealthy Shoulder Handbook: 100 Exercises for Treating and Preventing Frozen Shoulder, Rotator Cuff and other Common InjuriesРейтинг: 2 из 5 звезд2/5 (1)
- Ankle Sprain Rehabilitation ProgramДокумент4 страницыAnkle Sprain Rehabilitation Programkarep89949Оценок пока нет
- Pro Quest DocumentsДокумент47 страницPro Quest Documentsvothihongnga05vtОценок пока нет
- ClubfootДокумент5 страницClubfootCherry AlmarezОценок пока нет
- Total Knee ReplacementДокумент35 страницTotal Knee ReplacementYumi Kaito100% (3)
- Stretching-From Top To Bottom: Real Detroit MuscleДокумент9 страницStretching-From Top To Bottom: Real Detroit MuscleViyaan Singh GurjarОценок пока нет
- Rotator Cuff Tears - Symptoms, Causes, Diagnosis and TreatmentДокумент19 страницRotator Cuff Tears - Symptoms, Causes, Diagnosis and TreatmentsafiraОценок пока нет
- Fikri Zulfikar Najat - Ilmu Keolahragaan - Report TextДокумент4 страницыFikri Zulfikar Najat - Ilmu Keolahragaan - Report TextFikri Zulfikar NajatОценок пока нет
- Ligaments HipДокумент5 страницLigaments HipRizka Kartikasari100% (1)
- What Is A Fractured FemurДокумент16 страницWhat Is A Fractured FemurMaricris DatinguinooОценок пока нет
- How To Fix Flat Feet (Pes Planus) - Posture Direct PDFДокумент77 страницHow To Fix Flat Feet (Pes Planus) - Posture Direct PDFBosco DominicОценок пока нет
- ScoliosisДокумент8 страницScoliosisShanada JulistiadizenОценок пока нет
- What You Should Know About Shoulder InstabilityДокумент4 страницыWhat You Should Know About Shoulder InstabilityWoo Guan Lee100% (1)
- ScoliosisДокумент25 страницScoliosisshanel18100% (1)
- The Cast and SplintsДокумент18 страницThe Cast and Splintshatem alsrour100% (2)
- OrthoДокумент4 страницыOrthokelvinkurtОценок пока нет
- Wrist Injury at SiteДокумент10 страницWrist Injury at SiteClark Angelo JuanОценок пока нет
- Kneecap DislocationДокумент2 страницыKneecap DislocationbiancaОценок пока нет
- Hip DislocationДокумент4 страницыHip DislocationcrunkestОценок пока нет
- CT CastCareДокумент2 страницыCT CastCareLaira CañeteОценок пока нет
- TM_ SPORTS MEDICINE PATIENT ADVISOR - PERONEAL TENDON STRAINДокумент15 страницTM_ SPORTS MEDICINE PATIENT ADVISOR - PERONEAL TENDON STRAINYuni FridayaniОценок пока нет
- Hip Pain: Treating Hip Pain: Preventing Hip Pain, All Natural Remedies For Hip Pain, Medical Cures For Hip Pain, Along With Exercises And Rehab For Hip Pain ReliefОт EverandHip Pain: Treating Hip Pain: Preventing Hip Pain, All Natural Remedies For Hip Pain, Medical Cures For Hip Pain, Along With Exercises And Rehab For Hip Pain ReliefОценок пока нет
- CRI 089 Midterm NotesДокумент39 страницCRI 089 Midterm Notesdebroah280Оценок пока нет
- CASTДокумент4 страницыCASTAlliah OrdanОценок пока нет
- Mobility AidsДокумент80 страницMobility AidsVaraОценок пока нет
- What Are The Types of Injuries? What Is The Proper Treatment? When Should I Call EMS?Документ6 страницWhat Are The Types of Injuries? What Is The Proper Treatment? When Should I Call EMS?zimahnordinОценок пока нет
- Guide To Ankle InstabilityДокумент2 страницыGuide To Ankle Instabilityfahmiatul lailiОценок пока нет
- Management of Bone InjuriesДокумент13 страницManagement of Bone InjuriesKURIMAONGОценок пока нет
- O o o o o o o o O: Home Contact UsДокумент4 страницыO o o o o o o o O: Home Contact UsshaneОценок пока нет
- KT TAPE English InstructionsДокумент24 страницыKT TAPE English InstructionsAlexandra ComanОценок пока нет
- Taking Action To Reduce Back PainДокумент1 страницаTaking Action To Reduce Back PainSkalliburОценок пока нет
- Electrolyte BalanceДокумент4 страницыElectrolyte BalanceRaul NoceteОценок пока нет
- DMC Sparkle Water RefillingДокумент19 страницDMC Sparkle Water RefillingRaul Nocete100% (3)
- DMC Sparkle Water RefillingДокумент19 страницDMC Sparkle Water RefillingRaul Nocete100% (3)
- Anatomy and Physiology of the Nervous SystemДокумент2 страницыAnatomy and Physiology of the Nervous SystemRaul NoceteОценок пока нет
- Anatomy and Physiology of the Nervous SystemДокумент2 страницыAnatomy and Physiology of the Nervous SystemRaul NoceteОценок пока нет
- CystolithiasisДокумент7 страницCystolithiasisRaul Nocete100% (1)
- HCC PathophysioДокумент2 страницыHCC PathophysioRaul NoceteОценок пока нет
- Credit LectureДокумент18 страницCredit LectureRaul NoceteОценок пока нет
- Management Orientation LectureДокумент45 страницManagement Orientation LectureRaul NoceteОценок пока нет