Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- MCPS Sports Concussion Data 2014-15Документ1 страницаMCPS Sports Concussion Data 2014-15Concussion_MCPS_MdОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Parent Letter To MCPS Re Student Injury Data - 01-14-2015Документ11 страницParent Letter To MCPS Re Student Injury Data - 01-14-2015Concussion_MCPS_MdОценок пока нет
- Brain Sentry Inova Football Helmet Sensor Research Study ProposalДокумент5 страницBrain Sentry Inova Football Helmet Sensor Research Study ProposalConcussion_MCPS_MdОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- NFL 2010 Letter Re Concussion LegДокумент2 страницыNFL 2010 Letter Re Concussion LegConcussion_MCPS_MdОценок пока нет
- MCPS (MD) Tobacco-Free SCH PolicyДокумент2 страницыMCPS (MD) Tobacco-Free SCH PolicyConcussion_MCPS_MdОценок пока нет
- Template 3-A, MCPS Athletics Injury Report Each High School (From Athletic Trainer Data)Документ1 страницаTemplate 3-A, MCPS Athletics Injury Report Each High School (From Athletic Trainer Data)Concussion_MCPS_MdОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- MCPS Student Injury Report FormДокумент2 страницыMCPS Student Injury Report FormConcussion_MCPS_MdОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
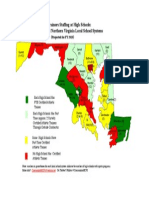
- Projected Ath Trainer HS Staffing in FY 2015-Map of MD and N. VA CountiesДокумент1 страницаProjected Ath Trainer HS Staffing in FY 2015-Map of MD and N. VA CountiesConcussion_MCPS_MdОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- MD Bill - HS Football Helmet Sensor Pilot ProgramДокумент6 страницMD Bill - HS Football Helmet Sensor Pilot ProgramConcussion_MCPS_MdОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Tabla 2023-1Документ31 страницаTabla 2023-1Pedro NavajaОценок пока нет
- Physical EducationДокумент224 страницыPhysical EducationHItesh Patre100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Last Sunset of SummerДокумент748 страницThe Last Sunset of SummerVhea Christine GuatnoОценок пока нет
- Readworks PassageДокумент4 страницыReadworks Passageapi-325026134Оценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Menlo College Special Teams OverviewДокумент14 страницMenlo College Special Teams OverviewCoach Brown100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Relationshipbetween Ownership Structureand Club Performanceinthe EPLДокумент19 страницThe Relationshipbetween Ownership Structureand Club Performanceinthe EPLCB19K069川名裕樹Оценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Documentation Centre 148418 v1 Technicalreportandstatistics Fifau 20worldcupcanada2007 28313Документ210 страницDocumentation Centre 148418 v1 Technicalreportandstatistics Fifau 20worldcupcanada2007 28313Nico OleaОценок пока нет
- Global Marketing & E-CommerceДокумент25 страницGlobal Marketing & E-CommerceKIRTI PATELОценок пока нет
- Luyen Nghe Anh 6 + File NgheДокумент4 страницыLuyen Nghe Anh 6 + File NgheHoàng Mạnh CườngОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Iowa Sports Connection 2011 Pigskin Preview EditionДокумент75 страницThe Iowa Sports Connection 2011 Pigskin Preview EditionISCEditorОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Registration FormДокумент12 страницRegistration FormRitesh JainОценок пока нет
- The Rover - Part 1 - 2016/17 Melchester Rovers SeasonДокумент18 страницThe Rover - Part 1 - 2016/17 Melchester Rovers SeasonCyril "Storky" KnightОценок пока нет
- Guidelines For 5000mДокумент7 страницGuidelines For 5000mAdina Elena ȘОценок пока нет
- Henrik - TFTL Character Sheet PDFДокумент1 страницаHenrik - TFTL Character Sheet PDFDeclan FeeneyОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Baylor Man To Man Quick HittersДокумент17 страницBaylor Man To Man Quick Hittersfercole100% (1)
- Suzuki sj410 Workshop Manual PDFДокумент4 страницыSuzuki sj410 Workshop Manual PDFAditya Hendra0% (4)
- IFBB Pro Beverly DiRenzo Passes Away at Age 49 - Fitness VoltДокумент14 страницIFBB Pro Beverly DiRenzo Passes Away at Age 49 - Fitness VoltRonald MoelkerОценок пока нет
- The Synonymy of Balance and Motion: by Doug Gray, FAFSДокумент3 страницыThe Synonymy of Balance and Motion: by Doug Gray, FAFSCris CavasottoОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Model Test Paper 2Документ26 страницModel Test Paper 2Faridah ShazlinaОценок пока нет
- Slovin's Formula: NCR Population 18 Years Old and AboveДокумент10 страницSlovin's Formula: NCR Population 18 Years Old and AboveKarl Joshua HernandezОценок пока нет
- Family Fortunes PDFДокумент2 страницыFamily Fortunes PDFHermione GrangerОценок пока нет
- Mosaic Trd1 U3 CeДокумент1 страницаMosaic Trd1 U3 CepersonalzОценок пока нет
- P.E 3Документ9 страницP.E 3Krisel TadtadОценок пока нет
- Phil Longo Developing QBs in Air RaidДокумент24 страницыPhil Longo Developing QBs in Air RaidGBO98Оценок пока нет
- Resistance Band Work OutДокумент9 страницResistance Band Work OutJulyyyОценок пока нет
- Plank Progression - Wk1-Wk4Документ4 страницыPlank Progression - Wk1-Wk4jakeОценок пока нет
- A Quiver To Hunt WithДокумент5 страницA Quiver To Hunt WithfedericopitopitoОценок пока нет
- Localized VolleyballДокумент30 страницLocalized VolleyballSharmaine Joy Naraja MicuaОценок пока нет
- GMS - QuestionárioДокумент84 страницыGMS - QuestionárioVitor SilvestreОценок пока нет
- ENG - PRE AFF ManualДокумент29 страницENG - PRE AFF ManualdrGunjanОценок пока нет