Вам также может понравиться
- Incoterms Chart of Responsibility 2020 1Документ1 страницаIncoterms Chart of Responsibility 2020 1Hiro Katsumoto100% (1)
- SAP MM Functional OverviewДокумент124 страницыSAP MM Functional OverviewRahul V GopinathОценок пока нет
- Care Coordination: - Case Management - Disease ManagementДокумент27 страницCare Coordination: - Case Management - Disease Managementamarneh1969Оценок пока нет
- The COAT & Review Approach: How to recognise and manage unwell patientsОт EverandThe COAT & Review Approach: How to recognise and manage unwell patientsРейтинг: 5 из 5 звезд5/5 (1)
- ENA Leadership Conference 2013 ProgramДокумент17 страницENA Leadership Conference 2013 ProgramEmergency Nurses AssociationОценок пока нет
- PROJECT CHARTER Pressure UlcerДокумент2 страницыPROJECT CHARTER Pressure UlcerQuality PmnhОценок пока нет
- Ways To Improve The Health SystemДокумент18 страницWays To Improve The Health SystemB I N SОценок пока нет
- Gap Report Astha HospitalДокумент49 страницGap Report Astha HospitalNidhi VijanОценок пока нет
- KPI Discussion Paper 3Документ22 страницыKPI Discussion Paper 3Manager HR Hijaz Hospital100% (1)
- Hospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsОт EverandHospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsОценок пока нет
- 2010 Patient Care Tracer Surgery or 1Документ6 страниц2010 Patient Care Tracer Surgery or 1Dutz Serrano100% (1)
- NPS - Patient Feedback FormДокумент1 страницаNPS - Patient Feedback FormNatasha BhasinОценок пока нет
- Quality Manager Job Description - 09-13Документ3 страницыQuality Manager Job Description - 09-13DrSaswat LincolnОценок пока нет
- Departmental Nursing Orientation ChecklistДокумент2 страницыDepartmental Nursing Orientation ChecklistMero Hassan50% (2)
- MODULE 3 STUDENT National Patient Safety Goals 2013Документ15 страницMODULE 3 STUDENT National Patient Safety Goals 2013Dewi Ratna Sari100% (1)
- CBAHI PresentationДокумент23 страницыCBAHI PresentationPrince Jhessie L. AbellaОценок пока нет
- 13 Patient Saefty and Quality ImprovementДокумент36 страниц13 Patient Saefty and Quality ImprovementShafiq Ur RahmanОценок пока нет
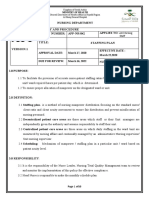
- APP Staffing PlanДокумент10 страницAPP Staffing PlanMADEL CAGARA DONDOYANOОценок пока нет
- IPSG PresentationДокумент38 страницIPSG Presentationmuhammed shamaa100% (1)
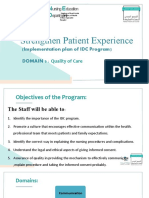
- Strengthen Patient Experience: (Implementation Plan of IDC Program) Domain 3Документ17 страницStrengthen Patient Experience: (Implementation Plan of IDC Program) Domain 3Rina LestariОценок пока нет
- AK Purchase and Disbursement CycleДокумент7 страницAK Purchase and Disbursement CyclecykenОценок пока нет
- Annual Appraisal 2019 EДокумент2 страницыAnnual Appraisal 2019 EPrince Jhessie L. AbellaОценок пока нет
- Deficiencies Observed During Pre-Assessment - Paf 2 Hospital (Full Accreditation) : Date(s) of VisitДокумент8 страницDeficiencies Observed During Pre-Assessment - Paf 2 Hospital (Full Accreditation) : Date(s) of Visitpranit mОценок пока нет
- LeadershipДокумент17 страницLeadershipHadi Mohammed HamedОценок пока нет
- CBAHI and JCI Common Asked Questions. 2023Документ5 страницCBAHI and JCI Common Asked Questions. 2023Rini NoviantiОценок пока нет
- NABH Awareness Program: Training DocumentДокумент12 страницNABH Awareness Program: Training DocumentquasysОценок пока нет
- Caselet 1 Pi Foods LTD - Managing Sales and DistributionДокумент3 страницыCaselet 1 Pi Foods LTD - Managing Sales and DistributionshivamОценок пока нет
- Orientation Program For New Nurses in Emergency DepartmentДокумент38 страницOrientation Program For New Nurses in Emergency DepartmentNers SenОценок пока нет
- Your Quarterly Bill: How To PayДокумент2 страницыYour Quarterly Bill: How To PayPaul ClimasОценок пока нет
- QA For Radiology DepartmentДокумент3 страницыQA For Radiology DepartmentRaviraj Pishe100% (1)
- NABH AdvantageДокумент19 страницNABH Advantagedr_vikasОценок пока нет
- Obeid Specialized Hospital - Riyadh: Quality Indicator Form 2018 2019Документ2 страницыObeid Specialized Hospital - Riyadh: Quality Indicator Form 2018 2019LovelydePerioОценок пока нет
- Medication Competency Assessment MC002Документ48 страницMedication Competency Assessment MC002Ameng GosimОценок пока нет
- 2.2.4. Eye Health Clinical Audit - Indicators List: Section One: Primary Eye Care ChecksДокумент2 страницы2.2.4. Eye Health Clinical Audit - Indicators List: Section One: Primary Eye Care ChecksCynthia Jaramillo MachucaОценок пока нет
- Hospital GuidelinesДокумент236 страницHospital GuidelinesMheanne Romano100% (1)
- Challenges For AccreditationДокумент22 страницыChallenges For AccreditationMohammad Muntaz AliОценок пока нет
- Auditing and Corporate Governance-JurazДокумент47 страницAuditing and Corporate Governance-JurazShami100% (3)
- Quality Introduction: Performance IndicatorДокумент28 страницQuality Introduction: Performance IndicatorLiza VarouqaОценок пока нет
- كيف تجتاز jciДокумент379 страницكيف تجتاز jciwaleed fangaryОценок пока нет
- CHAP 10. Internal Control and Control RiskДокумент27 страницCHAP 10. Internal Control and Control RiskNoro100% (1)
- CQE 7 Nursing Quality Indicators 1Документ24 страницыCQE 7 Nursing Quality Indicators 1Inder Singh YadavОценок пока нет
- Vital Signs and Early Warning ScoresДокумент47 страницVital Signs and Early Warning Scoresdr_nadheem100% (1)
- Product Version: Boost Up Your Certification ScoreДокумент6 страницProduct Version: Boost Up Your Certification ScoreMOHD PERFECT100% (1)
- Joint Commission International: Nepomuceno, Rose Ann TДокумент42 страницыJoint Commission International: Nepomuceno, Rose Ann TRoan Nepomuceno - Joaquin100% (1)
- 2 Process Addresses Discharge of All Patients Including Medico-Legal Cases and Patients Leaving Against Medical Advice.Документ6 страниц2 Process Addresses Discharge of All Patients Including Medico-Legal Cases and Patients Leaving Against Medical Advice.Sanjay Kadam100% (1)
- Patient SafetyДокумент27 страницPatient Safetyarahman168Оценок пока нет
- Assessment and Re-Assessment of Patients According To The Scope of ServiceДокумент9 страницAssessment and Re-Assessment of Patients According To The Scope of Servicegiya nursingОценок пока нет
- Nursing Self Assessment ToolkitДокумент19 страницNursing Self Assessment ToolkitJasmeet KaurОценок пока нет
- IPSG JCIA Measurable Elements and IntentsДокумент4 страницыIPSG JCIA Measurable Elements and IntentsHana Sanchez AlobaidanОценок пока нет
- Seminar JCI - 9 Feb 2012Документ16 страницSeminar JCI - 9 Feb 2012Mahardika PertiwiОценок пока нет
- Daftar Panduan JCIДокумент12 страницDaftar Panduan JCIEko Wahyu AgustinОценок пока нет
- 4+Roadmap+to+NABH+ +finalДокумент18 страниц4+Roadmap+to+NABH+ +finalSameer BugdeОценок пока нет
- RMO Assessment Form 2016Документ8 страницRMO Assessment Form 2016Tp HoangОценок пока нет
- NABH 3rd EditionДокумент258 страницNABH 3rd EditionAnuj Jindal100% (2)
- Hospital Safety OfficerДокумент1 страницаHospital Safety OfficerSalvador Morales Obusan100% (1)
- Homoeopathy Indicators NABHДокумент105 страницHomoeopathy Indicators NABHMamoni MaityОценок пока нет
- Medical Superintendent JobДокумент1 страницаMedical Superintendent JobJoshua AbhishekОценок пока нет
- Patient Satisfaction QuestionnaireДокумент4 страницыPatient Satisfaction QuestionnairePrasad KVVОценок пока нет
- Clinical AuditДокумент5 страницClinical AuditdrskumarОценок пока нет
- MedicineДокумент19 страницMedicineSarah100% (1)
- Infection Control Bundles For HospitalДокумент12 страницInfection Control Bundles For HospitalumeshbhartiОценок пока нет
- D125: Demo of NABH Hospital Accreditation Document Kit: Price 699 USDДокумент16 страницD125: Demo of NABH Hospital Accreditation Document Kit: Price 699 USDSandipan GhoshОценок пока нет
- ICAP Basic ICRA With MatrixДокумент4 страницыICAP Basic ICRA With MatrixmiptahulОценок пока нет
- Annual Health Check Up FormДокумент1 страницаAnnual Health Check Up FormNayan RoychowdhuryОценок пока нет
- JCI Standards Interpretation - June12004Документ18 страницJCI Standards Interpretation - June12004Niharika SharmaОценок пока нет
- Enhancing Nurses Pain Assessment To Improve.11Документ2 страницыEnhancing Nurses Pain Assessment To Improve.11Na d'Nazaie CodeОценок пока нет
- Healthcare Environmental Services A Complete Guide - 2020 EditionОт EverandHealthcare Environmental Services A Complete Guide - 2020 EditionОценок пока нет
- Patient Safety Organization A Complete Guide - 2020 EditionОт EverandPatient Safety Organization A Complete Guide - 2020 EditionОценок пока нет
- Bank of Punjab ATM EnglishДокумент43 страницыBank of Punjab ATM EnglishphooolОценок пока нет
- HSBC Amanah Debit Card-I & CNPДокумент2 страницыHSBC Amanah Debit Card-I & CNPNic CheongОценок пока нет
- Rini Mam NotesДокумент15 страницRini Mam NotesasbroadwayОценок пока нет
- s68 PDFДокумент2 страницыs68 PDFAnthemBeatsОценок пока нет
- Issued By: Go Air: Nikitha Online Services R04AG3006Документ2 страницыIssued By: Go Air: Nikitha Online Services R04AG3006NIKITHA ONLINESERVICESОценок пока нет
- Verification of TransciptДокумент1 страницаVerification of TransciptSdffОценок пока нет
- Revenue Cycle Conceptual SystemДокумент7 страницRevenue Cycle Conceptual SystemLil ConicОценок пока нет
- Administrate Network and Hardware PeripheralsvДокумент45 страницAdministrate Network and Hardware Peripheralsvmelkamu endaleОценок пока нет
- Ioe CN Lab 3Документ5 страницIoe CN Lab 3creatophileОценок пока нет
- Osmania University: (Scan QR Code With QR Reader To Know The Transaction Status)Документ1 страницаOsmania University: (Scan QR Code With QR Reader To Know The Transaction Status)minhajuddin kmОценок пока нет
- Engleski I I II PDFДокумент23 страницыEngleski I I II PDFvejnicОценок пока нет
- Justinas Kaminskas PMДокумент1 страницаJustinas Kaminskas PMapi-182285162Оценок пока нет
- DRAP New Rules On Ethical Marketing To HCPsДокумент10 страницDRAP New Rules On Ethical Marketing To HCPsRaheel KhanОценок пока нет
- Online Mcqs Test - Mobile Computing MCQ With AnswersДокумент1 страницаOnline Mcqs Test - Mobile Computing MCQ With AnswershiОценок пока нет
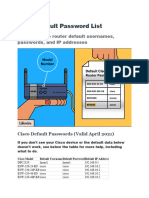
- Cisco Default Password ListДокумент5 страницCisco Default Password ListSiles Sandel100% (1)
- Sample CTC WorkingДокумент2 страницыSample CTC WorkingWall Street Forex (WSFx)Оценок пока нет
- Core SI RFP Volume IДокумент354 страницыCore SI RFP Volume ImrudrabhОценок пока нет
- Informed Delivery Sign Up GuideДокумент6 страницInformed Delivery Sign Up GuideONSITEОценок пока нет
- Review of Related Literature and StudiesДокумент7 страницReview of Related Literature and StudiesGlaiza GanoОценок пока нет
- Assignment: Software Defined Networking (SDN)Документ12 страницAssignment: Software Defined Networking (SDN)Rosemelyne WartdeОценок пока нет
- Reserch Final-2Документ76 страницReserch Final-2Kalkidan ZerihunОценок пока нет
- Exercise Week 6Документ5 страницExercise Week 6amirahhani najmaОценок пока нет