Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- 100 IdeasДокумент21 страница100 IdeasNo ID100% (1)
- Intraoperative RecordДокумент2 страницыIntraoperative Recordademaala06100% (1)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Snatch - Biomech Breakdown and Rapid Mastery Training Sequence, The - Eric WongДокумент38 страницSnatch - Biomech Breakdown and Rapid Mastery Training Sequence, The - Eric Wongcoachhand100% (4)
- The Body MechanicДокумент66 страницThe Body Mechaniccoachhand97% (31)
- 10 Commandments of Powerlifting - Ernie FrantzДокумент153 страницы10 Commandments of Powerlifting - Ernie Frantzcoachhand92% (12)
- Reloading DataДокумент72 страницыReloading DataWilhelm SwartОценок пока нет
- Cash Budget Sharpe Corporation S Projected Sales First 8 Month oДокумент1 страницаCash Budget Sharpe Corporation S Projected Sales First 8 Month oAmit PandeyОценок пока нет
- ETP Flexible Eating GuideДокумент61 страницаETP Flexible Eating Guidecoachhand100% (1)
- 2013 AUMF HearingДокумент58 страниц2013 AUMF HearingcoachhandОценок пока нет
- Armed Forces Ministry by MailДокумент1 страницаArmed Forces Ministry by MailcoachhandОценок пока нет
- Bulletproof Diet Road MapДокумент1 страницаBulletproof Diet Road MapLeRo2409Оценок пока нет
- Lutheran Veteran CertificateДокумент1 страницаLutheran Veteran CertificatecoachhandОценок пока нет
- Lutheran Prayer Guide For Those Who ServeДокумент23 страницыLutheran Prayer Guide For Those Who ServecoachhandОценок пока нет
- Latif Thomas Sprint Training - Inventory DemandsДокумент11 страницLatif Thomas Sprint Training - Inventory Demandscoachhand100% (3)
- USAF 30 Year Strategy - Directed Energy WeaponsДокумент22 страницыUSAF 30 Year Strategy - Directed Energy WeaponsMichael JanitchОценок пока нет
- Cutting WeightДокумент32 страницыCutting Weightcoachhand100% (2)
- BJJ Goal Setting GuideДокумент33 страницыBJJ Goal Setting Guidecoachhand100% (4)
- Cloud Computing PrimerДокумент19 страницCloud Computing PrimercoachhandОценок пока нет
- P4 Sniper ReticleДокумент1 страницаP4 Sniper ReticlecoachhandОценок пока нет
- Castle Doctrine and Self-Defense LawsДокумент44 страницыCastle Doctrine and Self-Defense LawscoachhandОценок пока нет
- Rage Fitness CatalogДокумент27 страницRage Fitness CatalogcoachhandОценок пока нет
- Rad Energy System TrainДокумент8 страницRad Energy System TraincoachhandОценок пока нет
- Combat LifesaverДокумент211 страницCombat LifesaverMisty D Cahal100% (1)
- Lean and Mean Blueprint ManualДокумент18 страницLean and Mean Blueprint Manualcoachhand100% (2)
- Asymmetric Warfare Group "Sniper Awareness and Counter Sniper Reference Card"Документ2 страницыAsymmetric Warfare Group "Sniper Awareness and Counter Sniper Reference Card"Impello_Tyrannis100% (11)
- Standard Reticle Patterns 2012Документ100 страницStandard Reticle Patterns 2012coachhand100% (1)
- Operation Urgent Fury GrenadaДокумент93 страницыOperation Urgent Fury GrenadacoachhandОценок пока нет
- Cyber Info SharingДокумент8 страницCyber Info SharingcoachhandОценок пока нет
- Robert E. Lee's SharpshootersДокумент499 страницRobert E. Lee's SharpshooterscoachhandОценок пока нет
- M&PtriggerjobДокумент46 страницM&PtriggerjobcoachhandОценок пока нет
- Elements of A Research ArgumentДокумент6 страницElements of A Research ArgumentcoachhandОценок пока нет
- Castle Doctrine and Self-Defense LawsДокумент44 страницыCastle Doctrine and Self-Defense LawscoachhandОценок пока нет
- DOD-DHS Cybersecurity Memorandum of AgreementДокумент5 страницDOD-DHS Cybersecurity Memorandum of Agreementspencerackerman7502Оценок пока нет
- Vignyapan 18-04-2024Документ16 страницVignyapan 18-04-2024adil1787Оценок пока нет
- The Global Entrepreneurship and Development Index 2014 For Web1 PDFДокумент249 страницThe Global Entrepreneurship and Development Index 2014 For Web1 PDFAlex Yuri Rodriguez100% (1)
- PDFДокумент3 страницыPDFvaliОценок пока нет
- Acronyms and AbbreviationsДокумент875 страницAcronyms and AbbreviationsLacky KrishnanОценок пока нет
- NIFT GAT Sample Test Paper 1Документ13 страницNIFT GAT Sample Test Paper 1goelОценок пока нет
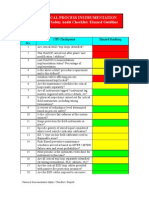
- Chemical Safety ChecklistДокумент3 страницыChemical Safety ChecklistPillai Sreejith100% (10)
- Cs Fujitsu SAP Reference Book IPDFДокумент63 страницыCs Fujitsu SAP Reference Book IPDFVijay MindfireОценок пока нет
- The Dust Bunnies COL FKBДокумент36 страницThe Dust Bunnies COL FKBPradeep ManralОценок пока нет
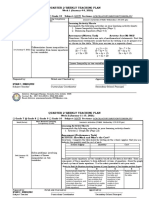
- Teaching Plan - Math 8 Week 1-8 PDFДокумент8 страницTeaching Plan - Math 8 Week 1-8 PDFRYAN C. ENRIQUEZОценок пока нет
- Topic 6 Nested For LoopsДокумент21 страницаTopic 6 Nested For Loopsthbull02Оценок пока нет
- DISTRICT CENSUS HANDBOOK North GoaДокумент190 страницDISTRICT CENSUS HANDBOOK North Goants1020Оценок пока нет
- Book Review Fiction New HereДокумент7 страницBook Review Fiction New HereFILZAH SYAUQINA BINTI SUBLY Pelajar KPTM IpohОценок пока нет
- Cuentos CADEДокумент6 страницCuentos CADEMäuricio E. González VegaОценок пока нет
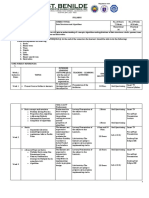
- Data Structures and Algorithms SyllabusДокумент9 страницData Structures and Algorithms SyllabusBongbong GalloОценок пока нет
- API IND DS2 en Excel v2 10081834Документ462 страницыAPI IND DS2 en Excel v2 10081834Suvam PatelОценок пока нет
- Ch04Exp PDFДокумент17 страницCh04Exp PDFConstantin PopescuОценок пока нет
- Useful Methods in CatiaДокумент30 страницUseful Methods in CatiaNastase Corina100% (2)
- Catalogo HydronixДокумент68 страницCatalogo HydronixNANCHO77Оценок пока нет
- Overview of Incorporation in CambodiaДокумент3 страницыOverview of Incorporation in CambodiaDavid MОценок пока нет
- CBSE Class 10 Science Sample Paper SA 2 Set 1Документ5 страницCBSE Class 10 Science Sample Paper SA 2 Set 1Sidharth SabharwalОценок пока нет
- CCNP SWITCH 300-115 - Outline of The Official Study GuideДокумент31 страницаCCNP SWITCH 300-115 - Outline of The Official Study GuidehammiesinkОценок пока нет
- Grade 10 Module 1 Performing Roughing in Activities For Communication and DistributДокумент26 страницGrade 10 Module 1 Performing Roughing in Activities For Communication and DistributNelshane JohnОценок пока нет
- Letter of Acceptfor TДокумент3 страницыLetter of Acceptfor TCCSОценок пока нет
- Onco Case StudyДокумент2 страницыOnco Case StudyAllenОценок пока нет
- Adigrat University: College of Engineering and Technology Department of Chemical EnginneringДокумент39 страницAdigrat University: College of Engineering and Technology Department of Chemical EnginneringSeid Aragaw100% (1)
- Polyembryony &its ImportanceДокумент17 страницPolyembryony &its ImportanceSURIYA PRAKASH GОценок пока нет
- TSC M34PV - TSC M48PV - User Manual - CryoMed - General Purpose - Rev A - EnglishДокумент93 страницыTSC M34PV - TSC M48PV - User Manual - CryoMed - General Purpose - Rev A - EnglishMurielle HeuchonОценок пока нет