Вам также может понравиться
- Smart Women - Foolish WomenДокумент96 страницSmart Women - Foolish Womenedghiun100% (1)
- Sexual Mastery System - Robert IrwinДокумент79 страницSexual Mastery System - Robert IrwinmuooziОценок пока нет
- Excursie DubaiДокумент14 страницExcursie DubaiedghiunОценок пока нет
- PJL Ebook Hoopono FinalДокумент82 страницыPJL Ebook Hoopono FinaledghiunОценок пока нет
- 8 Section Brocade Chi GongДокумент81 страница8 Section Brocade Chi Gongedghiun100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- 6-Drugs Acting On The Renal System - 2Документ65 страниц6-Drugs Acting On The Renal System - 2Hamid Hussain HamidОценок пока нет
- FCPS Part 1 Medicine 186 QuestionsДокумент11 страницFCPS Part 1 Medicine 186 QuestionsServantof IslamОценок пока нет
- Diuretics 140628134114 Phpapp02Документ45 страницDiuretics 140628134114 Phpapp02P merugu100% (1)
- Final Exam Review - Bio 172Документ21 страницаFinal Exam Review - Bio 172Erin McElhaney QuirkОценок пока нет
- Diuretic DrugsДокумент16 страницDiuretic DrugslabillabooОценок пока нет
- Lse 05Документ26 страницLse 05Anjali MunjalОценок пока нет
- Grade 11 Life Sciences Revision Material Term 3 and 4 - 2023Документ41 страницаGrade 11 Life Sciences Revision Material Term 3 and 4 - 2023Junior NgwenyaОценок пока нет
- 33 MCQs On Renal Physiology USMLE Step 1 ForumДокумент23 страницы33 MCQs On Renal Physiology USMLE Step 1 ForumAisha YolaОценок пока нет
- Unit 5 Respiration, Internal Environment, Coordination and Gene TechnologyДокумент55 страницUnit 5 Respiration, Internal Environment, Coordination and Gene TechnologyMaha NaserОценок пока нет
- The Whole Enchilada PDFДокумент602 страницыThe Whole Enchilada PDFMr XОценок пока нет
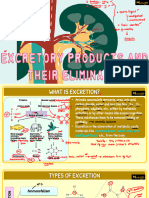
- NCERT Solutions For Class 11 Biology Chapter 19: Excretory Products and Their Elimination Class 11Документ6 страницNCERT Solutions For Class 11 Biology Chapter 19: Excretory Products and Their Elimination Class 11HarshitОценок пока нет
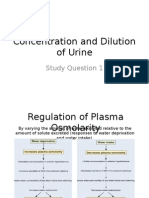
- Concentration and Dilution of UrineДокумент20 страницConcentration and Dilution of UrineNeil Alcantara SantiОценок пока нет
- Tubular Reabsorption & SecretionДокумент25 страницTubular Reabsorption & SecretionRishabh DangiОценок пока нет
- All Quiz QuestionsДокумент60 страницAll Quiz QuestionsMorgan ChristОценок пока нет
- QP BT Jam2022Документ28 страницQP BT Jam2022Kumar KalyanОценок пока нет
- Fluid and Electrolyte Balance ReportДокумент10 страницFluid and Electrolyte Balance ReportYani ManuelОценок пока нет
- 19.3.2 KidneyДокумент77 страниц19.3.2 KidneyDak AnneОценок пока нет
- BB3102-WPI Exam3 PrepДокумент4 страницыBB3102-WPI Exam3 PrepLiz MillerОценок пока нет
- Practice Questions For Function of The Urinary System-AnswersДокумент16 страницPractice Questions For Function of The Urinary System-AnswersDebra Gan100% (1)
- Urinary System15Документ47 страницUrinary System15Michael John PaderesОценок пока нет
- Vipin Sir Biology 19. Excretory Products and Their EliminationДокумент55 страницVipin Sir Biology 19. Excretory Products and Their EliminationvanshpatelssisОценок пока нет
- Bio-Zoology - Vol - 2 EM PDFДокумент176 страницBio-Zoology - Vol - 2 EM PDFmuraliОценок пока нет
- Counter Current MechanismДокумент21 страницаCounter Current MechanismAdnan BasheerОценок пока нет
- Anatomic and Physiologic OverviewДокумент5 страницAnatomic and Physiologic OverviewShannen Alija M. LaoОценок пока нет
- Nephrolithiasis CPДокумент54 страницыNephrolithiasis CPSheena VallesОценок пока нет
- BiologyДокумент16 страницBiologyShivansh NayakОценок пока нет
- Kidney FunctionДокумент64 страницыKidney FunctionVincent LivandyОценок пока нет
- Module 17 - Urinary SystemДокумент18 страницModule 17 - Urinary SystemSam TagardaОценок пока нет
- Case PresentationДокумент39 страницCase PresentationAnni BarbaОценок пока нет
- Cheat Sheet ExamsДокумент5 страницCheat Sheet ExamsSwe LayОценок пока нет