Вам также может понравиться
- Liver Curs 2009Документ215 страницLiver Curs 2009Mohammad_Islam87Оценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- AnaemiaДокумент83 страницыAnaemiaMohammad_Islam87100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Lecture 20 CarcinogenesisДокумент84 страницыLecture 20 CarcinogenesisMohammad_Islam87100% (1)
- Morphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadДокумент19 страницMorphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadMohammad_Islam87Оценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
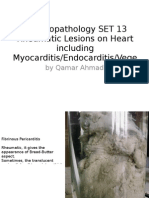
- Morphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeДокумент25 страницMorphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeMohammad_Islam87Оценок пока нет
- Morphopathology SET 15 Renal Pathologies: by Qamar AhmadДокумент25 страницMorphopathology SET 15 Renal Pathologies: by Qamar AhmadMohammad_Islam87Оценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Morphopathology SET 16 Pathologies of The Gastrointestinal TractДокумент29 страницMorphopathology SET 16 Pathologies of The Gastrointestinal TractMohammad_Islam87Оценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Borcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarДокумент7 страницBorcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Morphopathology SET14 Respiratory Pathologies: by Qamar AhmadДокумент18 страницMorphopathology SET14 Respiratory Pathologies: by Qamar AhmadMohammad_Islam87Оценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
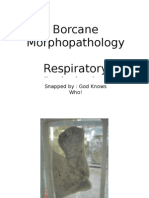
- Borcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarДокумент11 страницBorcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Оценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Workshop 20Документ2 страницыWorkshop 20Mohammad_Islam87Оценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Borcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarДокумент7 страницBorcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Оценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Morphopathology Macroscopy (Romanian-Batch)Документ187 страницMorphopathology Macroscopy (Romanian-Batch)Mohammad_Islam87100% (1)
- ?#ry%oefr: - J4 @,8/ MryДокумент15 страниц?#ry%oefr: - J4 @,8/ MryMohammad_Islam87Оценок пока нет
- Morphopatholgy Set 9 Circulatory Disturbances: by Qamar AhmadДокумент24 страницыMorphopatholgy Set 9 Circulatory Disturbances: by Qamar AhmadMohammad_Islam87Оценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Physical Signs of The AbdomenДокумент93 страницыPhysical Signs of The AbdomenaimanОценок пока нет
- Macroscopy Set 10 Circulatory Disturbances: by Qamar AhmadДокумент55 страницMacroscopy Set 10 Circulatory Disturbances: by Qamar AhmadMohammad_Islam87Оценок пока нет
- Workshop 19Документ3 страницыWorkshop 19Mohammad_Islam87Оценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Morphopathology Set 11 Atherosclerosis and Other Cardiaovascular DisordersДокумент21 страницаMorphopathology Set 11 Atherosclerosis and Other Cardiaovascular DisordersMohammad_Islam87Оценок пока нет
- Conditions Presenting With Abdominal PainДокумент69 страницConditions Presenting With Abdominal PainaimanОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Examination of AbdomenДокумент41 страницаExamination of AbdomenMohammad_Islam87Оценок пока нет
- Workshop 18Документ4 страницыWorkshop 18Mohammad_Islam87Оценок пока нет
- Stomach - GastritisДокумент22 страницыStomach - GastritisaimanОценок пока нет
- Workshop 17Документ4 страницыWorkshop 17Mohammad_Islam87Оценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Morphopathology Set 8 Melanocytic Tumors: by Qamar AhmadДокумент54 страницыMorphopathology Set 8 Melanocytic Tumors: by Qamar AhmadMohammad_Islam87Оценок пока нет
- Peptic Ulcer DiseaseДокумент54 страницыPeptic Ulcer DiseaseMohammad_Islam87Оценок пока нет
- STOMACCURS2Документ12 страницSTOMACCURS2Mohammad_Islam87Оценок пока нет
- Eeh455 Assignment2b MaharpДокумент22 страницыEeh455 Assignment2b Maharpapi-267478292Оценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Polscience 6th SemДокумент16 страницPolscience 6th Semritam1994paulОценок пока нет
- Fractures NoteДокумент31 страницаFractures NoteNoor AlblushiОценок пока нет
- SIPДокумент2 страницыSIPRowena Abdula BaronaОценок пока нет
- The Ethics of Helping Transgender Men and Women Have ChildrenДокумент16 страницThe Ethics of Helping Transgender Men and Women Have ChildrenAnonymous 75M6uB3OwОценок пока нет
- NARQ40007-PROCESS - Beauty Parlor ManagementДокумент3 страницыNARQ40007-PROCESS - Beauty Parlor ManagementYogesh ThakurОценок пока нет
- Worm The Game Edit of Wildbow'sДокумент16 страницWorm The Game Edit of Wildbow'sLuke AjemОценок пока нет
- Seminar and Topic ObjectivesДокумент2 страницыSeminar and Topic ObjectivesNeyo KatalbasОценок пока нет
- Aquatics AssignmentДокумент12 страницAquatics AssignmentTyrone WewpOgzОценок пока нет
- Physical Fitness Test Individual Score CardДокумент12 страницPhysical Fitness Test Individual Score CardJunessa TadinaОценок пока нет
- Medical Terminology Worksheet-2Документ4 страницыMedical Terminology Worksheet-2pumpiepumpkin12Оценок пока нет
- Family and Community Profile I. General InformationДокумент4 страницыFamily and Community Profile I. General InformationMary Leour PascuaОценок пока нет
- Development of A Taste-Masked Orodispersible FilmДокумент12 страницDevelopment of A Taste-Masked Orodispersible FilmKhoa DuyОценок пока нет
- Hafiz Fizalia - Acupuncture Hack - The Easiest Way To Learn Classical Theories of Acupuncture (2018) PDFДокумент66 страницHafiz Fizalia - Acupuncture Hack - The Easiest Way To Learn Classical Theories of Acupuncture (2018) PDFkhalid Sijilmassi100% (3)
- Potsdam Village Police Dept. Blotter Sept. 10, 2017Документ2 страницыPotsdam Village Police Dept. Blotter Sept. 10, 2017NewzjunkyОценок пока нет
- Clinical Practice Guidelines: High-Grade Glioma: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpДокумент9 страницClinical Practice Guidelines: High-Grade Glioma: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpSiva SubramaniamОценок пока нет
- Angelman Syndrome - Identification and ManagementДокумент10 страницAngelman Syndrome - Identification and ManagementFajar YuniftiadiОценок пока нет
- Body Template 1998Документ7 страницBody Template 1998itayОценок пока нет
- HeartДокумент12 страницHeartRebar photographyОценок пока нет
- Treatment and Prognosis of Febrile Seizures - UpToDateДокумент14 страницTreatment and Prognosis of Febrile Seizures - UpToDateDinointernosОценок пока нет
- Bleeding During Pregnancy and Nursing Care PlanДокумент17 страницBleeding During Pregnancy and Nursing Care PlanLizcelle Bihasa86% (7)
- Paper On Rag PickersДокумент11 страницPaper On Rag PickershsrapsОценок пока нет
- Registrars Manual On Band DДокумент32 страницыRegistrars Manual On Band DkailasasundaramОценок пока нет
- Summarised Clinchers Created For The Exam - Credits - Audi Maglalang-ReedДокумент9 страницSummarised Clinchers Created For The Exam - Credits - Audi Maglalang-ReedflashjetОценок пока нет
- OpdscheduleДокумент14 страницOpdscheduleSrinidhi ChandraguthiОценок пока нет
- Nitroimidazole Wps OfficeДокумент10 страницNitroimidazole Wps OfficeCamelle DiniayОценок пока нет
- STD.: Xi Practice Test - 2016 Date: 0 14 - 10 - 2016 SUBJECT: Zoology Animal HusbandryДокумент2 страницыSTD.: Xi Practice Test - 2016 Date: 0 14 - 10 - 2016 SUBJECT: Zoology Animal HusbandryDr-Atin Kumar SrivastavaОценок пока нет
- How To File A Claim-For GSISДокумент2 страницыHow To File A Claim-For GSISZainal Abidin AliОценок пока нет
- 2022 Projects City of BethlehemДокумент17 страниц2022 Projects City of BethlehemLVNewsdotcomОценок пока нет
- Skin and Soft Tissue Injuries & InfectionsДокумент221 страницаSkin and Soft Tissue Injuries & InfectionsMario Espinosa100% (1)