Вам также может понравиться
- Mitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsОт EverandMitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsОценок пока нет
- Cardiogenic Shock: Sparsh Goel 77Документ28 страницCardiogenic Shock: Sparsh Goel 77Sparsh GoelОценок пока нет
- Myocarditis, (Inflamed Heart Muscles) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandMyocarditis, (Inflamed Heart Muscles) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Clinical Cases in Right Heart FailureОт EverandClinical Cases in Right Heart FailureLana TsaoОценок пока нет
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsОт EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsОценок пока нет
- Problem-based Approach to Gastroenterology and HepatologyОт EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisОценок пока нет
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsОт EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsОценок пока нет
- Perioperative Medicine: Medical Consultation and Co-managementОт EverandPerioperative Medicine: Medical Consultation and Co-managementAmir K. JafferОценок пока нет
- The Pathophysiology and Pharmacotherapy of Myocardial InfarctionОт EverandThe Pathophysiology and Pharmacotherapy of Myocardial InfarctionNabil El-SherifОценок пока нет
- Night Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandNight Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- A Nurse's Guide to Caring for Cardiac Intervention PatientsОт EverandA Nurse's Guide to Caring for Cardiac Intervention PatientsОценок пока нет
- Anticoagulants ParamedДокумент20 страницAnticoagulants ParamedManikanta GupthaОценок пока нет
- Congestive Heart FailureДокумент12 страницCongestive Heart FailureyvasparksОценок пока нет
- ABC of Heart FailureДокумент4 страницыABC of Heart Failurekunalprabhu148Оценок пока нет
- CPG - Pneumonia (2010 Update)Документ55 страницCPG - Pneumonia (2010 Update)Jade Kenneth Gonzales LomansocОценок пока нет
- Heart Failure - AhaДокумент77 страницHeart Failure - AhaChendy Endriansa100% (1)
- Ascites Hrs B WPДокумент101 страницаAscites Hrs B WPGhias Un Nabi TayyabОценок пока нет
- Generic Name Therapeutic Classification Pharmacologic ClassificationДокумент3 страницыGeneric Name Therapeutic Classification Pharmacologic ClassificationAnselle CasilОценок пока нет
- Trials SummaryДокумент12 страницTrials SummaryReda SoОценок пока нет
- PericarditisДокумент29 страницPericarditisPavin KumarОценок пока нет
- Cardio Notes, Heart FailureДокумент17 страницCardio Notes, Heart FailureJoy DunwanОценок пока нет
- 25 Cardiovascular DiseaseДокумент35 страниц25 Cardiovascular DiseaseBramantyo NugrosОценок пока нет
- Ch-13 Drugs Used in Heart FailureДокумент49 страницCh-13 Drugs Used in Heart FailureShabrin SadikhОценок пока нет
- Hypertension LecturesДокумент65 страницHypertension LecturesAdebisiОценок пока нет
- Cardiac PathophysiologyДокумент83 страницыCardiac PathophysiologyJauhar Anindita SariОценок пока нет
- Mechanical Circulatory Support OverviewДокумент34 страницыMechanical Circulatory Support OverviewJohn100% (1)
- Atrial Fibrillation: Presented by ShehzadiДокумент17 страницAtrial Fibrillation: Presented by ShehzadisamОценок пока нет
- Ultimate Reference DocumentДокумент29 страницUltimate Reference DocumentShellyza Moledina SajwaniОценок пока нет
- 2019 - MCardiology - Clinical Features of Val HT 2019 2Документ72 страницы2019 - MCardiology - Clinical Features of Val HT 2019 2Vaenusha MuruganОценок пока нет
- HF2019Документ24 страницыHF2019Sima Noviantika100% (2)
- HemodialysisДокумент6 страницHemodialysisAnonymous 7LI78gu4VDОценок пока нет
- Electrolyte DisordersДокумент10 страницElectrolyte DisordersSlavicaОценок пока нет
- Cardiogenic ShockДокумент49 страницCardiogenic Shockp.sanОценок пока нет
- ACE InhibitorsДокумент26 страницACE Inhibitorsali mohammedОценок пока нет
- Congestive Heart FailureДокумент86 страницCongestive Heart FailureNabeel ShahzadОценок пока нет
- The Lower Respiratory Tract Infection: Pneumonia: Ida Bagus Ngurah RaiДокумент32 страницыThe Lower Respiratory Tract Infection: Pneumonia: Ida Bagus Ngurah RaiFelicia adeline ChristianОценок пока нет
- Congestive Heart FailureДокумент19 страницCongestive Heart FailureIlavenil PanduranganОценок пока нет
- Dapa CKDДокумент11 страницDapa CKDCarlos Andres Tejeda PerezОценок пока нет
- Use of Vasopressors and Inotropes - UpToDateДокумент18 страницUse of Vasopressors and Inotropes - UpToDateAlbertoMarteОценок пока нет
- Renal Replacement Therapy in Acute Kidney Injury 2017Документ14 страницRenal Replacement Therapy in Acute Kidney Injury 2017piero reyes100% (1)
- Blood, Coagulation of Blood & Bleeding Disorders 12 - 7 - 19Документ62 страницыBlood, Coagulation of Blood & Bleeding Disorders 12 - 7 - 19AntarleenaОценок пока нет
- Types of ArrhythmiaДокумент10 страницTypes of ArrhythmiaRonilyn Mae AlvarezОценок пока нет
- 29744226: Cerebral Pathophysiology in Extracorporeal Membrane Oxygenation Pitfalls in Daily Clinical ManagementДокумент11 страниц29744226: Cerebral Pathophysiology in Extracorporeal Membrane Oxygenation Pitfalls in Daily Clinical ManagementEward Rod SalОценок пока нет
- Approach To Ventricular ArrhythmiasДокумент18 страницApproach To Ventricular ArrhythmiasDavid CruzОценок пока нет
- Atelectasis: Contraction Atelectasis (Or Cicatrization Atelectasis)Документ10 страницAtelectasis: Contraction Atelectasis (Or Cicatrization Atelectasis)Gan BangОценок пока нет
- Essential Hypertension ManagementДокумент5 страницEssential Hypertension Managementspicychips7Оценок пока нет
- PR BleedДокумент20 страницPR BleedCathy KayОценок пока нет
- Cardiac (Heart) FailureДокумент27 страницCardiac (Heart) FailureSanthoshi Sadhanaa SankarОценок пока нет
- Renal - Replacement - TherapyДокумент128 страницRenal - Replacement - TherapyEmОценок пока нет
- The BreastДокумент72 страницыThe BreastMohammad_Islam87Оценок пока нет
- Physiopathology SyllabusДокумент1 страницаPhysiopathology SyllabusMohammad_Islam87Оценок пока нет
- Lecture 17 DiabetesДокумент51 страницаLecture 17 DiabetesMohammad_Islam87Оценок пока нет
- Lecture 18 Upper Digestive DiseasesДокумент63 страницыLecture 18 Upper Digestive DiseasesMohammad_Islam87Оценок пока нет
- The LymphomasДокумент46 страницThe LymphomasMohammad_Islam87Оценок пока нет
- Lecture 20 CarcinogenesisДокумент84 страницыLecture 20 CarcinogenesisMohammad_Islam87100% (1)
- Pharmacology Lecture 12-5-2009, OpiodsДокумент18 страницPharmacology Lecture 12-5-2009, OpiodsMohammad_Islam87Оценок пока нет
- Curst Um Abd EnglДокумент10 страницCurst Um Abd EnglMohammad_Islam87Оценок пока нет
- Abdominal HerniaeДокумент66 страницAbdominal HerniaeMohammad_Islam87Оценок пока нет
- Plastic SurgeryДокумент11 страницPlastic SurgeryMohammad_Islam87Оценок пока нет
- Liver Curs 2009Документ215 страницLiver Curs 2009Mohammad_Islam87Оценок пока нет
- ?#ry%oefr: - J4 @,8/ MryДокумент15 страниц?#ry%oefr: - J4 @,8/ MryMohammad_Islam87Оценок пока нет
- AnaemiaДокумент83 страницыAnaemiaMohammad_Islam87100% (2)
- Pharmacology Lecture 19-5-2009, NSAIDSДокумент19 страницPharmacology Lecture 19-5-2009, NSAIDSMohammad_Islam87Оценок пока нет
- Borcane TumorДокумент14 страницBorcane TumorMohammad_Islam87Оценок пока нет
- Morphopathology SET 15 Renal Pathologies: by Qamar AhmadДокумент25 страницMorphopathology SET 15 Renal Pathologies: by Qamar AhmadMohammad_Islam87Оценок пока нет
- Morphopathology SET 16 Pathologies of The Gastrointestinal TractДокумент29 страницMorphopathology SET 16 Pathologies of The Gastrointestinal TractMohammad_Islam87Оценок пока нет
- Morphopathology Macroscopy (Romanian-Batch)Документ187 страницMorphopathology Macroscopy (Romanian-Batch)Mohammad_Islam87100% (1)
- Morphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadДокумент19 страницMorphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadMohammad_Islam87Оценок пока нет
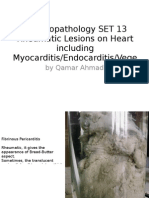
- Morphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeДокумент25 страницMorphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeMohammad_Islam87Оценок пока нет
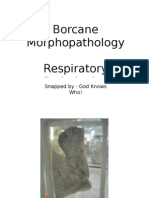
- Borcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarДокумент11 страницBorcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Оценок пока нет
- Borcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarДокумент7 страницBorcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87100% (1)
- Pharmacology Lecture Diuretic Agents (High Quality)Документ15 страницPharmacology Lecture Diuretic Agents (High Quality)Mohammad_Islam87Оценок пока нет
- Morphopathology SET14 Respiratory Pathologies: by Qamar AhmadДокумент18 страницMorphopathology SET14 Respiratory Pathologies: by Qamar AhmadMohammad_Islam87Оценок пока нет
- Borcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarДокумент7 страницBorcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Оценок пока нет
- Workshop 20Документ2 страницыWorkshop 20Mohammad_Islam87Оценок пока нет
- Pharmacology Lecture 5-5-2009Документ15 страницPharmacology Lecture 5-5-2009Mohammad_Islam87Оценок пока нет
- Conditions Presenting With Abdominal PainДокумент69 страницConditions Presenting With Abdominal PainaimanОценок пока нет
- Workshop 19Документ3 страницыWorkshop 19Mohammad_Islam87Оценок пока нет
- Engl BUN - EditДокумент167 страницEngl BUN - EditMohammad_Islam87Оценок пока нет
- Circulatory and Respiratory System Crossword PuzzleДокумент4 страницыCirculatory and Respiratory System Crossword Puzzlejoel jacobОценок пока нет
- Hagiwara, 2017Документ13 страницHagiwara, 2017luccafcms56Оценок пока нет
- Daftar Pustaka: Medical Students and Faculty - Edisi Keempat - Baltimore-PhiladelpiaДокумент2 страницыDaftar Pustaka: Medical Students and Faculty - Edisi Keempat - Baltimore-PhiladelpiaSylvia PertiwiОценок пока нет
- Patofisiologi Sistem KardiovaskularДокумент157 страницPatofisiologi Sistem KardiovaskularNyanmaruОценок пока нет
- Aortic DissectionДокумент5 страницAortic DissectionCosminNGDNОценок пока нет
- Avant Review Lesson 1-8 ECG Rhythm Strip InterpretationДокумент28 страницAvant Review Lesson 1-8 ECG Rhythm Strip InterpretationphoebjaetanОценок пока нет
- Lesson 4 - Circulatory SystemДокумент21 страницаLesson 4 - Circulatory SystemJoseeОценок пока нет
- Management of Severe Hypertension, Hypertension in Special ConditionДокумент43 страницыManagement of Severe Hypertension, Hypertension in Special Conditionabhandlung100% (3)
- Presentor: DR - Kumar Moderator: DR - VamsidharДокумент71 страницаPresentor: DR - Kumar Moderator: DR - VamsidharJayaprakash KuppusamyОценок пока нет
- Cardiac Cycle JVPДокумент70 страницCardiac Cycle JVPAstrid PramudyaaОценок пока нет
- Ischaemia of Lower Limbs: by Dr. ShampileДокумент46 страницIschaemia of Lower Limbs: by Dr. ShampileFreeburn SimunchembuОценок пока нет
- Correlation Seminar On Cardiovascular SystemДокумент20 страницCorrelation Seminar On Cardiovascular Systemnischal neupaneОценок пока нет
- 2021 IC + Injuria RenalДокумент16 страниц2021 IC + Injuria RenalAndjela KosticОценок пока нет
- P1 MS 3 Nur 200Документ16 страницP1 MS 3 Nur 200Xandra Joie Ondoy TabotaboОценок пока нет
- Policies and Statements: Peripheral Arterial UltrasoundДокумент5 страницPolicies and Statements: Peripheral Arterial UltrasoundJing CruzОценок пока нет
- Terapi Oksigen Terhadap Perubahan Saturasi Oksigen Melalui Pemeriksaan Oksimetri Pada Pasien Infark Miokard Akut (Ima)Документ6 страницTerapi Oksigen Terhadap Perubahan Saturasi Oksigen Melalui Pemeriksaan Oksimetri Pada Pasien Infark Miokard Akut (Ima)edi sambasОценок пока нет
- Ehy340 PDFДокумент83 страницыEhy340 PDFghufran adnanОценок пока нет
- Overview Beta BlockersДокумент11 страницOverview Beta BlockersginafujiОценок пока нет
- Arteriovenous Fistula (Avf) Monitoring and Surveillance: SciencedirectДокумент5 страницArteriovenous Fistula (Avf) Monitoring and Surveillance: SciencedirectFarid RakhmanОценок пока нет
- HypertensionДокумент2 страницыHypertensionRodel Yacas0% (1)
- Atherosclerosis CompendiumДокумент13 страницAtherosclerosis CompendiumanushanОценок пока нет
- Coronary AngioplastyДокумент2 страницыCoronary AngioplastySiti Hasmah JamilОценок пока нет
- Starling ForcesДокумент1 страницаStarling ForcesbernieОценок пока нет
- JAtin ProjectДокумент9 страницJAtin ProjectAnonymousОценок пока нет
- Falenissa - Pemicu 3 Blok Etika Dan Hukum KedokteranДокумент108 страницFalenissa - Pemicu 3 Blok Etika Dan Hukum KedokteranIcarus WingsОценок пока нет
- Deep Vein ThrombosisДокумент16 страницDeep Vein ThrombosisB1 TutorialОценок пока нет
- 33 Characteristics and Comorbidities Of.33Документ2 страницы33 Characteristics and Comorbidities Of.33rizkydarmawangmailОценок пока нет
- Tromboembolismo Pulmonar Manejo PDFДокумент7 страницTromboembolismo Pulmonar Manejo PDFGeovannaHGОценок пока нет
- Pengetahuan, Sikap, Dan Perilaku Terhadap Pencegahan Serta Penanggulangan Hipertensi Di Kabupaten BogorДокумент9 страницPengetahuan, Sikap, Dan Perilaku Terhadap Pencegahan Serta Penanggulangan Hipertensi Di Kabupaten BogorIntan OktavianiОценок пока нет
- Utility of Endoscopic Ultrasound in Symptomatic Cut Corners of A ClotДокумент3 страницыUtility of Endoscopic Ultrasound in Symptomatic Cut Corners of A ClotDjabhi SpinzzОценок пока нет