Вам также может понравиться
- A Stepwise Approach To Acid Base Disorders in ICUДокумент71 страницаA Stepwise Approach To Acid Base Disorders in ICUVishal Prabhu100% (3)
- Approach: A. How The Kidney Handle The Proteins?Документ9 страницApproach: A. How The Kidney Handle The Proteins?Rashed ShatnawiОценок пока нет
- Treatment of Resistant and Refractory HypertensionДокумент21 страницаTreatment of Resistant and Refractory HypertensionLuis Rodriguez100% (1)
- Core V - Cardiovascular CoreДокумент35 страницCore V - Cardiovascular CoreMatthew LeiОценок пока нет
- Normal Impulse Conduction and ECG InterpretationДокумент73 страницыNormal Impulse Conduction and ECG InterpretationIndra ToshiwayОценок пока нет
- CardiologyДокумент149 страницCardiologyMuhammad SyafiqОценок пока нет
- Cardiology Guide: Key Concepts, Formulas and Treatment StrategiesДокумент5 страницCardiology Guide: Key Concepts, Formulas and Treatment StrategiesRodrigo FonsecaОценок пока нет
- H&P GuideДокумент7 страницH&P GuideTBWPОценок пока нет
- Suspecting Pulmonary Hypertension in The Dyspneic Patient: Who, When, and HowДокумент92 страницыSuspecting Pulmonary Hypertension in The Dyspneic Patient: Who, When, and HowJonathan LongОценок пока нет
- ECG Interpretation DR - Rawan AlshreemДокумент25 страницECG Interpretation DR - Rawan AlshreemMarymii Al-sahlawiiОценок пока нет
- Aorta DissectionДокумент98 страницAorta DissectionDian SukaryaОценок пока нет
- ECG IMM 2020.docx.2Документ25 страницECG IMM 2020.docx.2Abdul QuyyumОценок пока нет
- Critical Decisions in Emergency and Acute Care ElectrocardiographyОт EverandCritical Decisions in Emergency and Acute Care ElectrocardiographyОценок пока нет
- Pediatric Cardiology LectureДокумент87 страницPediatric Cardiology LectureMena HashemОценок пока нет
- VALVULAR HEART DISEASE GUIDEДокумент69 страницVALVULAR HEART DISEASE GUIDEAbanoub AwadallaОценок пока нет
- Ecg Tutorial PDFДокумент82 страницыEcg Tutorial PDFpacpacpac123Оценок пока нет
- Er Medicine ReviewДокумент16 страницEr Medicine Reviewsdb10cОценок пока нет
- Free Medical ECG Interpretation PresentationsДокумент30 страницFree Medical ECG Interpretation PresentationsRohini SelvarajahОценок пока нет
- Critical Care: ElectrophysiologyДокумент180 страницCritical Care: ElectrophysiologyArianne Joy C. TamarayОценок пока нет
- Adult Congenital Heart Disease Board ReviewДокумент79 страницAdult Congenital Heart Disease Board ReviewKhajornsak Som-UnОценок пока нет
- Basic ECG Interpretation MWДокумент211 страницBasic ECG Interpretation MWLorelie AsisОценок пока нет
- ECG Learning ModulesДокумент150 страницECG Learning ModulesdodiОценок пока нет
- PANCE Prep Pearls Valvular Disease PDFДокумент4 страницыPANCE Prep Pearls Valvular Disease PDFkatОценок пока нет
- AbgДокумент52 страницыAbgm07wwpОценок пока нет
- Clinical Tips in Cardiovascular EmergenciesДокумент86 страницClinical Tips in Cardiovascular EmergenciesAbdul Quyyum100% (3)
- One Stop Doc Immunology - Stewart, John, Sadler, AmyДокумент153 страницыOne Stop Doc Immunology - Stewart, John, Sadler, AmyCosmin NeaguОценок пока нет
- Sepsis Update 2019Документ44 страницыSepsis Update 2019Yeshwanth Umapathi100% (1)
- Short Cases in Clinical Exams of Internal Medicine (PDFDrive)Документ185 страницShort Cases in Clinical Exams of Internal Medicine (PDFDrive)Nadhirah ZulkifliОценок пока нет
- Heartbeat Irregularities ExplainedДокумент5 страницHeartbeat Irregularities ExplainedKayelyn-Rose Combate100% (1)
- Cardiology Clinic 2006Документ620 страницCardiology Clinic 2006JoNykolasОценок пока нет
- Mitral StenosisДокумент29 страницMitral Stenosisrameshbmc100% (4)
- Rheumatic Fever and Rheumatic Heart DiseaseДокумент54 страницыRheumatic Fever and Rheumatic Heart DiseaseFian AldyОценок пока нет
- Cardiac ArrestДокумент42 страницыCardiac ArrestAlyssandra LucenoОценок пока нет
- Pathophysiology of Myocardial InfarctionДокумент2 страницыPathophysiology of Myocardial Infarctionkobe_andre15100% (28)
- Internal MedicineДокумент185 страницInternal MedicineFarah FarahОценок пока нет
- Pediatrics ECG by DR Ali Bel KheirДокумент9 страницPediatrics ECG by DR Ali Bel KheirFerasОценок пока нет
- HTA Europeo PDFДокумент675 страницHTA Europeo PDFFrancisco Javier Palma P100% (1)
- Disasters and Mass Casualty Incidents: The Nuts and Bolts of Preparedness and Response to Protracted and Sudden Onset EmergenciesОт EverandDisasters and Mass Casualty Incidents: The Nuts and Bolts of Preparedness and Response to Protracted and Sudden Onset EmergenciesMauricio LynnОценок пока нет
- 1 Acute Inferior Wall MI With First Degree BlockДокумент53 страницы1 Acute Inferior Wall MI With First Degree BlockKarthik KannappanОценок пока нет
- Hypertension NCLEX Quiz Questions: A. I Will Make Sure I Consume Foods High in PotassiumДокумент5 страницHypertension NCLEX Quiz Questions: A. I Will Make Sure I Consume Foods High in PotassiumMelodia Turqueza GandezaОценок пока нет
- STEMI Equivalents: DR Elesia Powell-Williams Emergency Medicine Resident PGY3Документ39 страницSTEMI Equivalents: DR Elesia Powell-Williams Emergency Medicine Resident PGY3elesia powell100% (1)
- Normal Ecg, Infarction & Arrhythmia SДокумент98 страницNormal Ecg, Infarction & Arrhythmia SAdinda GupitaОценок пока нет
- PRES MCQsДокумент218 страницPRES MCQsdoctorbilalsОценок пока нет
- Avnrt VS AvrtДокумент79 страницAvnrt VS AvrtDwi Nugroho PrastowoОценок пока нет
- Dr. Smith's ECG Blog - "Shark Fin" - A Deadly ECG Sign That You Must Know! PDFДокумент7 страницDr. Smith's ECG Blog - "Shark Fin" - A Deadly ECG Sign That You Must Know! PDFZACHARIAH MANKIRОценок пока нет
- Braunwald Lecture Series #2Документ33 страницыBraunwald Lecture Series #2usfcards100% (2)
- FRACP Recall Paper 2002: Part A - 70 Questions, 2 HoursДокумент43 страницыFRACP Recall Paper 2002: Part A - 70 Questions, 2 HoursZH. omg sarОценок пока нет
- Pearls and Pitfalls in The Crashing Geriatric PatientДокумент12 страницPearls and Pitfalls in The Crashing Geriatric PatientVikrantОценок пока нет
- ECG Interpretation in One PageДокумент2 страницыECG Interpretation in One PageRyan AycockОценок пока нет
- Diagnosis and Management of The Neonate With Critical Congenital Heart DiseaseДокумент35 страницDiagnosis and Management of The Neonate With Critical Congenital Heart Diseasemotzco0% (1)
- Cardiology IДокумент112 страницCardiology IAhmad Makhlouf100% (1)
- Fluids&Lytes PediatricДокумент33 страницыFluids&Lytes Pediatricnugraha_esaОценок пока нет
- Critical Care 2012Документ490 страницCritical Care 2012Carlos PradoОценок пока нет
- Murray CaseStudiesInNephrologyДокумент179 страницMurray CaseStudiesInNephrologyAdil BilaeloОценок пока нет
- 3 Minute EM Student PresentationДокумент5 страниц3 Minute EM Student Presentationdebra_euromОценок пока нет
- Pulmo ThromboembolismДокумент34 страницыPulmo ThromboembolismAlexander Santiago ParelОценок пока нет
- ECG Localization of Culprit Artery in Acute Myocardial InfarctionДокумент104 страницыECG Localization of Culprit Artery in Acute Myocardial Infarctionginaul100% (1)
- CV for Medical SpecialistДокумент8 страницCV for Medical SpecialistElena DumitriuОценок пока нет
- Ventricular Arrhythmias: Robert J. Hariman, MDДокумент51 страницаVentricular Arrhythmias: Robert J. Hariman, MDusfcardsОценок пока нет
- It sJustAQuizДокумент24 страницыIt sJustAQuizPrerna SehgalОценок пока нет
- Internal Medicine Topic List 2015Документ3 страницыInternal Medicine Topic List 2015Krystal Mae LopezОценок пока нет
- Mcqs On Reactive Lymphadenitis: 1) Reactive Follicular Hyperplasia Is Characterized byДокумент5 страницMcqs On Reactive Lymphadenitis: 1) Reactive Follicular Hyperplasia Is Characterized byAbdelrahman SwilamОценок пока нет
- Tetralogy of Fallot RadiologyДокумент13 страницTetralogy of Fallot RadiologyErlan Anugrah PratamaОценок пока нет
- Stemi ChecklistДокумент1 страницаStemi ChecklistDanu SusantoОценок пока нет
- Criterios de Barcelona 2020Документ22 страницыCriterios de Barcelona 2020Vallejo Romo Alberto CristianОценок пока нет
- EKG RhythmsДокумент71 страницаEKG RhythmsalexaОценок пока нет
- Structural CausesДокумент2 страницыStructural CausesAndo yuОценок пока нет
- 5 ECG Interpretation With AnswersДокумент48 страниц5 ECG Interpretation With AnswersQusai Ibraheem100% (1)
- Congenital Heart Disease Series 1Документ9 страницCongenital Heart Disease Series 1api-216828341Оценок пока нет
- CVS ExaminationДокумент85 страницCVS ExaminationPrasenjit DasОценок пока нет
- CardiovascularДокумент155 страницCardiovascularEric VeranoОценок пока нет
- Livia Sagita Ruslim Cardio StemiДокумент34 страницыLivia Sagita Ruslim Cardio StemiAnthony ChandraОценок пока нет
- ECG Exercises - Flutter Atrial 4:1 BlockДокумент5 страницECG Exercises - Flutter Atrial 4:1 BlockCuraj AliceОценок пока нет
- K31a - Electrophysiology and Cardiac Arrhytmia EmergencyДокумент46 страницK31a - Electrophysiology and Cardiac Arrhytmia EmergencyXeniel AlastairОценок пока нет
- 8 Heart and Neck Vessels AssessmentДокумент61 страница8 Heart and Neck Vessels AssessmentPrincess VanquirayОценок пока нет
- Article - CVD Cardiac Arrest - Bls AclsДокумент2 страницыArticle - CVD Cardiac Arrest - Bls AclsAkhosh SomarajanОценок пока нет
- Cardiogenic ShockДокумент42 страницыCardiogenic ShockpashaОценок пока нет
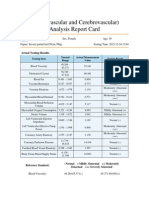
- Cardiovascular and CerebrovascularДокумент6 страницCardiovascular and CerebrovascularJoshelle B. Bancilo0% (1)
- Abdominal Aortic Aneurysm Diagnosis and ManagementДокумент49 страницAbdominal Aortic Aneurysm Diagnosis and ManagementGustavoJPereiraSОценок пока нет
- Stroke Dan Sepsis: Pembimbing: Dr. Bambang Supriadi, SP.SДокумент24 страницыStroke Dan Sepsis: Pembimbing: Dr. Bambang Supriadi, SP.SIcha NathaliaОценок пока нет
- Atrial Septal DefectДокумент3 страницыAtrial Septal Defectmu_crОценок пока нет
- DAFPUS Psikosomatis NewДокумент5 страницDAFPUS Psikosomatis NewEvy LiesniawatiОценок пока нет
- Normal EkgДокумент35 страницNormal EkgLau Song LungОценок пока нет