Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
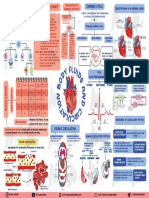
- A18 BODY FLUIDS in Human BodyДокумент1 страницаA18 BODY FLUIDS in Human Bodyservoculus machatteОценок пока нет
- Lesson 5 - Organs and Organ SystemsДокумент2 страницыLesson 5 - Organs and Organ SystemsnasrideviОценок пока нет
- Hematology: Shukur Wasman Smail PHD Student in ImmunologyДокумент12 страницHematology: Shukur Wasman Smail PHD Student in ImmunologyShukr Wesman BlbasОценок пока нет
- Grade 9 Quiz 2 LT2Документ1 страницаGrade 9 Quiz 2 LT2Ezekiel LapitanОценок пока нет
- Circulatory WksДокумент6 страницCirculatory WksPak RisОценок пока нет
- Tooth-Organ Relationship ChartДокумент1 страницаTooth-Organ Relationship ChartMichaelBrett100% (1)
- The Effect of Season On Sleep Patterns, Circadian Rhythms, and MoodДокумент20 страницThe Effect of Season On Sleep Patterns, Circadian Rhythms, and Mooddims expertОценок пока нет
- Medsci 142: Biology For Biomedical Science: Human Organ SystemsДокумент8 страницMedsci 142: Biology For Biomedical Science: Human Organ SystemsthefrenchnerdОценок пока нет
- ID Pengaruh Ukuran Manset Terhadap Hasil PeДокумент5 страницID Pengaruh Ukuran Manset Terhadap Hasil Pesiti hodijahОценок пока нет
- Transfusion ReactionsДокумент11 страницTransfusion ReactionsBungas Arisudana50% (2)
- L - Life Processes - Respiration Notes and Questions For Note Book WorkДокумент7 страницL - Life Processes - Respiration Notes and Questions For Note Book WorkNotImmortalОценок пока нет
- ABO Blood Group System PDFДокумент3 страницыABO Blood Group System PDFPerry Sin100% (1)
- 2nd Puc Biology Reasoning Questions ZoologyДокумент4 страницы2nd Puc Biology Reasoning Questions ZoologynomanОценок пока нет
- Anatomi Systema Respiratorium Dr. DodikДокумент58 страницAnatomi Systema Respiratorium Dr. DodikIrfan Maulana AjiОценок пока нет
- Tissue and Its ClassificationДокумент6 страницTissue and Its ClassificationPriyanjali Saini100% (1)
- Effectiveness of Deep Breathing Exercise On Blood Pressure Among Patients With Hypertension Ijariie5971Документ5 страницEffectiveness of Deep Breathing Exercise On Blood Pressure Among Patients With Hypertension Ijariie5971annaОценок пока нет
- TestReport - Apollo Main Hospital, Greams Road - 63b2aef9bb7ec962a187808bДокумент2 страницыTestReport - Apollo Main Hospital, Greams Road - 63b2aef9bb7ec962a187808bKumaran kumaranjОценок пока нет
- Fisiologi Sistem Saraf PusatДокумент90 страницFisiologi Sistem Saraf PusathardianОценок пока нет
- Science 9 - Circulatory SystemДокумент8 страницScience 9 - Circulatory SystemJames Russel MariОценок пока нет
- Sleeping Disorder ThesisДокумент7 страницSleeping Disorder Thesistsivhqvcf100% (2)
- Chrono Pharmaco L GyДокумент4 страницыChrono Pharmaco L GyRani SujithОценок пока нет
- Patient ProfileДокумент19 страницPatient Profilebangus08Оценок пока нет
- Reflexology Case Study - DiabetesДокумент13 страницReflexology Case Study - DiabetesSam Ruiz-Avila100% (2)
- Alterations in Respiratory FunctionsДокумент26 страницAlterations in Respiratory FunctionsAjeeshОценок пока нет
- Blood ChemistryДокумент28 страницBlood ChemistryAisha ShahfiqueeОценок пока нет
- G5summary of Endocrine System and Maintenance of The BodyДокумент15 страницG5summary of Endocrine System and Maintenance of The BodyNeil Ian Casuga TemblorОценок пока нет
- Blood PhysiologyДокумент35 страницBlood PhysiologyShane Margauxh AlabastroОценок пока нет
- Science Form 3 Blood Circulation and TransportДокумент8 страницScience Form 3 Blood Circulation and Transportkc_hani0% (1)
- Blood Product and Plasma SubstituentsДокумент14 страницBlood Product and Plasma SubstituentsDivya KMОценок пока нет
- ABO Blood GroupДокумент29 страницABO Blood GroupUpendra Sharma SulibeleОценок пока нет