Вам также может понравиться
- Astaxanthin Uses and Effectiveness in Therapy of Acnes Vulgaris Final Revisi 7Документ12 страницAstaxanthin Uses and Effectiveness in Therapy of Acnes Vulgaris Final Revisi 7Desica NatalisaОценок пока нет
- Conjunctivitis: by PGMI Jasleen MonrealДокумент77 страницConjunctivitis: by PGMI Jasleen MonrealJade MonrealОценок пока нет
- Derma NotesДокумент52 страницыDerma NotesUsmanОценок пока нет
- Corneal DiseasesДокумент32 страницыCorneal Diseasesnighat khanОценок пока нет
- Pathology of Eyelid, Conjunctiva and CorneaДокумент19 страницPathology of Eyelid, Conjunctiva and CorneaX And ZОценок пока нет
- Diseases of CorneaДокумент170 страницDiseases of CorneaLavanya MadabushiОценок пока нет
- ReferatДокумент31 страницаReferatrobby_94Оценок пока нет
- Dermatology Cutaneous Bacterial InfectionsДокумент139 страницDermatology Cutaneous Bacterial InfectionsArianne Joy C. TamarayОценок пока нет
- Eye DiseaseДокумент31 страницаEye DiseaseTsegaye YalewОценок пока нет
- Cellulitis: SHVNDR 1Документ13 страницCellulitis: SHVNDR 1Simran SinghОценок пока нет
- Vesiculobullous Lesions: Dr. Khushboo Kachhwaha, Reader, Dept. of Oral Medicine and RadiologyДокумент26 страницVesiculobullous Lesions: Dr. Khushboo Kachhwaha, Reader, Dept. of Oral Medicine and RadiologyHem pushp lata MewaraОценок пока нет
- Eyelid PathologyДокумент55 страницEyelid PathologyleahОценок пока нет
- Kuliah Mata Merah, Kelainan Struktur Dan Bentuk Mata - DR NaziyaДокумент47 страницKuliah Mata Merah, Kelainan Struktur Dan Bentuk Mata - DR NaziyaFastiati RAОценок пока нет
- Eye Diagnostic Points - McqsДокумент21 страницаEye Diagnostic Points - McqsMuhammad AwaisОценок пока нет
- Keratitis 09Документ29 страницKeratitis 09somebody_maОценок пока нет
- Tuberculosis: State The Possible Sites & Varied Clinical Presentations of Extra-Pulmonary TuberculosisДокумент15 страницTuberculosis: State The Possible Sites & Varied Clinical Presentations of Extra-Pulmonary TuberculosisDila MananОценок пока нет
- RED EYE WITH DECREASED VISION FixedДокумент70 страницRED EYE WITH DECREASED VISION FixedChandraОценок пока нет
- Diseases of The EyelidsДокумент9 страницDiseases of The EyelidsANTONIOОценок пока нет
- The CorneaДокумент60 страницThe CorneaSarahОценок пока нет
- Penyakit Pada MataДокумент138 страницPenyakit Pada Matadevi taqiyyahОценок пока нет
- Sread of InfectionДокумент7 страницSread of InfectionmustafaОценок пока нет
- Jogi - Hordoleum KalazionДокумент4 страницыJogi - Hordoleum KalazionhiОценок пока нет
- Vernal Keratoconjunctivitis: - Dr. Zulfiqar AliДокумент30 страницVernal Keratoconjunctivitis: - Dr. Zulfiqar AliAsad FrazОценок пока нет
- Cystic Orbital Lesions: 1. Dacryops 2. Dermoid CystДокумент9 страницCystic Orbital Lesions: 1. Dacryops 2. Dermoid CystAndriani Kemala SariОценок пока нет
- Tropical DiseasesДокумент44 страницыTropical DiseasesOsmanОценок пока нет
- Occur Largely in The Newborn and in Children Younger Than 5 Years, and Rarely in Older IndividualsДокумент6 страницOccur Largely in The Newborn and in Children Younger Than 5 Years, and Rarely in Older IndividualsElle ReyesОценок пока нет
- Chronic InfectionsДокумент60 страницChronic Infectionsnaveena reddyОценок пока нет
- Eye Adnexa Diseases: Catedra OftalmologieДокумент39 страницEye Adnexa Diseases: Catedra OftalmologieDanielaОценок пока нет
- Eye Diagnosis PointsДокумент50 страницEye Diagnosis PointsShoaib AkhtarОценок пока нет
- Affections of CorneaДокумент9 страницAffections of CorneaKirti JamwalОценок пока нет
- Conjunctiva Anatomy and PhysiologyДокумент106 страницConjunctiva Anatomy and Physiologysaddam0% (1)
- Recurrent: or Reinfection Susceptible People: Adult With Low Im Munity (Especially HIV Patient) Pathologic ChangesДокумент36 страницRecurrent: or Reinfection Susceptible People: Adult With Low Im Munity (Especially HIV Patient) Pathologic ChangesOsama SaidatОценок пока нет
- Conjunctivita - PPT (Lb. Engleza)Документ107 страницConjunctivita - PPT (Lb. Engleza)Ciubotaru CristiОценок пока нет
- Conjunctiva Anatomy and PhysiologyДокумент101 страницаConjunctiva Anatomy and PhysiologyPurva KeswaniОценок пока нет
- MK TuberculosisДокумент11 страницMK TuberculosisMoses Jr KazevuОценок пока нет
- Childhood TuberculosisДокумент59 страницChildhood TuberculosisVincent SerОценок пока нет
- Viral Diseases Newcastle Disease (ND)Документ47 страницViral Diseases Newcastle Disease (ND)thanh ba matОценок пока нет
- Kuliah Blok Mata: Halida Wibawaty Infection Immunology Subdivision Department of Ophthalmology RSUD DR Moewardi SurakartaДокумент51 страницаKuliah Blok Mata: Halida Wibawaty Infection Immunology Subdivision Department of Ophthalmology RSUD DR Moewardi SurakartaMuhammad Nur SidiqОценок пока нет
- Lichen PlanusДокумент6 страницLichen Planusأحمد عبد الوهابОценок пока нет
- Ocular Manifestations in AIDSДокумент27 страницOcular Manifestations in AIDSAnumeha Jindal100% (1)
- Mon Surgical Infections Boils, Abscess, Ulcer, Cellulitis, Curbuncle, Gangrene, Sinus, Fistula CДокумент48 страницMon Surgical Infections Boils, Abscess, Ulcer, Cellulitis, Curbuncle, Gangrene, Sinus, Fistula CPanna SahaОценок пока нет
- Keratitis KonjungtivitisДокумент81 страницаKeratitis KonjungtivitisAngnes Dera MustikaОценок пока нет
- Cutaneous TuberculosisДокумент78 страницCutaneous TuberculosisDr Daulat Ram DhakedОценок пока нет
- ConjunctivitisДокумент27 страницConjunctivitisGAURAVОценок пока нет
- Childhood TuberculosisДокумент60 страницChildhood TuberculosisyosephОценок пока нет
- Corneal Bacterial UlcerДокумент48 страницCorneal Bacterial UlcerAkansha Rastogi100% (1)
- Eyelids Diseases Lacrimal System DiseasesДокумент45 страницEyelids Diseases Lacrimal System DiseasesMAMA LALAОценок пока нет
- This Child Has Had A Sore Throat and Fever For 3 Days. The Appearance of The Throat Is Shown. What Do You See?Документ62 страницыThis Child Has Had A Sore Throat and Fever For 3 Days. The Appearance of The Throat Is Shown. What Do You See?Ivan KurniawanОценок пока нет
- Conjunctiva Anatomy and Physiology NewДокумент78 страницConjunctiva Anatomy and Physiology Newfachrie saputraОценок пока нет
- Diseases of The CorneaДокумент14 страницDiseases of The CorneaANTONIOОценок пока нет
- Extra-Cranial Complications of CSOMfinalДокумент37 страницExtra-Cranial Complications of CSOMfinalAarthi Gopal100% (2)
- 1.conjunctiva and ConjunctivitisДокумент77 страниц1.conjunctiva and ConjunctivitisPreeti PatelОценок пока нет
- KonjungtivitisДокумент46 страницKonjungtivitisBakri BayquniОценок пока нет
- Infeksi Kelainan Kongenital Dan TumorДокумент54 страницыInfeksi Kelainan Kongenital Dan Tumorniska darliantiОценок пока нет
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Документ48 страницP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Nauli PanjaitanОценок пока нет
- Red Eye With Normal VisionДокумент58 страницRed Eye With Normal VisionDiskaAstariniОценок пока нет
- Oral Cavity Malignancy-SurgeryДокумент62 страницыOral Cavity Malignancy-SurgeryAsif AbbasОценок пока нет
- Bacterial Infec2Документ17 страницBacterial Infec2Fazeela JamalОценок пока нет
- Cornea: Anatomy & PhysiologyДокумент68 страницCornea: Anatomy & Physiologyadeline0% (1)
- Vernal Keratoconjunctivitis (VKC)Документ19 страницVernal Keratoconjunctivitis (VKC)api-3742497Оценок пока нет
- Future Implications of Anti VegfДокумент6 страницFuture Implications of Anti VegfAnumeha JindalОценок пока нет
- ARMD StudyДокумент40 страницARMD StudyAnumeha JindalОценок пока нет
- Amsler's GridДокумент1 страницаAmsler's GridAnumeha JindalОценок пока нет
- Anti VegfДокумент3 страницыAnti VegfAnumeha Jindal100% (1)
- Amsler Grid 1Документ9 страницAmsler Grid 1Anumeha JindalОценок пока нет
- Inflammation in Dry Age Related Macular DegenrationДокумент11 страницInflammation in Dry Age Related Macular DegenrationAnumeha JindalОценок пока нет
- Micronutrients and AgeДокумент9 страницMicronutrients and AgeAnumeha JindalОценок пока нет
- ARMD GeneticsДокумент9 страницARMD GeneticsAnumeha JindalОценок пока нет
- Creating Your Own Blogger Template From Scratch, Sort ofДокумент11 страницCreating Your Own Blogger Template From Scratch, Sort ofAnumeha JindalОценок пока нет
- Flower Blossom Massage Oil RecipeДокумент1 страницаFlower Blossom Massage Oil RecipeAnumeha JindalОценок пока нет
- Age Related Macular DegenerationДокумент21 страницаAge Related Macular DegenerationAnumeha JindalОценок пока нет
- Essential Oil SubstitutesДокумент13 страницEssential Oil SubstitutesAnumeha JindalОценок пока нет
- Poster Design in CorelDrawДокумент72 страницыPoster Design in CorelDrawAnumeha Jindal50% (2)
- Exotic Massage Oil RecipeДокумент1 страницаExotic Massage Oil RecipeAnumeha JindalОценок пока нет
- Herbal Recipes For AromatherapyДокумент3 страницыHerbal Recipes For AromatherapyAnumeha Jindal100% (4)
- Exquisite Sandalwood Massage OilДокумент1 страницаExquisite Sandalwood Massage OilAnumeha JindalОценок пока нет
- From The Aromatherapy Recipe Files Volume 22Документ3 страницыFrom The Aromatherapy Recipe Files Volume 22Anumeha JindalОценок пока нет
- From The Aromatherapy Recipe Files Volume 21Документ3 страницыFrom The Aromatherapy Recipe Files Volume 21Anumeha JindalОценок пока нет
- Meditating With Essential OilsДокумент2 страницыMeditating With Essential OilsAnumeha JindalОценок пока нет
- From The Aromatherapy Recipe Files Volume 24Документ3 страницыFrom The Aromatherapy Recipe Files Volume 24Anumeha JindalОценок пока нет
- From The Aromatherapy Recipe Files Volume 20Документ3 страницыFrom The Aromatherapy Recipe Files Volume 20Anumeha JindalОценок пока нет
- How To Apply Essential Oils For Chakra BalancingДокумент2 страницыHow To Apply Essential Oils For Chakra BalancingAnumeha Jindal100% (1)
- From The Aromatherapy Recipe FilesДокумент2 страницыFrom The Aromatherapy Recipe FilesAnumeha JindalОценок пока нет
- Insomnia Relief Massage Oil RecipeДокумент1 страницаInsomnia Relief Massage Oil RecipeAnumeha JindalОценок пока нет
- The Third Eye (Brow) Chakra and Essential OilsДокумент2 страницыThe Third Eye (Brow) Chakra and Essential OilsAnumeha JindalОценок пока нет
- Some Substitutions For Essential OilsДокумент1 страницаSome Substitutions For Essential OilsAnumeha JindalОценок пока нет
- Recipes Using JojobaДокумент1 страницаRecipes Using JojobaAnumeha JindalОценок пока нет
- Other Aromatherapy RecpiesДокумент13 страницOther Aromatherapy RecpiesAnumeha JindalОценок пока нет
- The Chakras and Essential OilsДокумент10 страницThe Chakras and Essential OilsAnumeha Jindal100% (4)
- Essential Oil of The Month: SandlewoodДокумент2 страницыEssential Oil of The Month: SandlewoodAnumeha Jindal0% (1)
- Week 4 Hand Washing and Ppe - CincoДокумент3 страницыWeek 4 Hand Washing and Ppe - CincoShecana Rose CincoОценок пока нет
- WVSU COM Clinical Clerkship Survival Guide PDFДокумент100 страницWVSU COM Clinical Clerkship Survival Guide PDFRoendel Bustillo100% (3)
- Culture and HealthДокумент3 страницыCulture and HealthEstiloОценок пока нет
- Myth in OrthoДокумент7 страницMyth in Orthosurendra334Оценок пока нет
- DEMENTIAДокумент42 страницыDEMENTIAputri maharaniОценок пока нет
- Referat HIV AIDSДокумент13 страницReferat HIV AIDSoctaviena zakariaОценок пока нет
- MalpresentationДокумент16 страницMalpresentationAnghel CruzОценок пока нет
- Determinants of HealthДокумент30 страницDeterminants of HealthRuchi YadavОценок пока нет
- Lecture Note: Health Information Management I (Hit 111)Документ27 страницLecture Note: Health Information Management I (Hit 111)Usman Ahmad TijjaniОценок пока нет
- Cuong Vong - Resume - RevisedДокумент2 страницыCuong Vong - Resume - Revisedapi-300295160Оценок пока нет
- School StressДокумент24 страницыSchool StressShaheen Khan WarsiОценок пока нет
- Testicular PainДокумент16 страницTesticular PainkdwazirОценок пока нет
- Week 3 Session 1 - Knife CrimeДокумент26 страницWeek 3 Session 1 - Knife CrimeAlejandro CardonaОценок пока нет
- Aacn Critical CareДокумент40 страницAacn Critical Careapi-348346538Оценок пока нет
- Shimla Nursing College Annadale Bai BerbaiДокумент17 страницShimla Nursing College Annadale Bai Berbaigill priyaОценок пока нет
- Seretide Accuhaler Pi Au PDFДокумент24 страницыSeretide Accuhaler Pi Au PDFJing Yi LeongОценок пока нет
- Background Info.Документ3 страницыBackground Info.Moses V. GonzalesОценок пока нет
- Active VFC ProvidersДокумент50 страницActive VFC ProvidersClint AnthonyОценок пока нет
- KUsta PDFДокумент29 страницKUsta PDFTokekKompieОценок пока нет
- s9 Basic Life SupportДокумент27 страницs9 Basic Life SupportputuОценок пока нет
- EpidemiologyДокумент52 страницыEpidemiologyasdfsОценок пока нет
- Hematology: Thrombosis and The Antiphospholipid SyndromeДокумент2 страницыHematology: Thrombosis and The Antiphospholipid SyndromeYohanna YohannaОценок пока нет
- Assisting in Patients Undergoing A ThoracentesisДокумент7 страницAssisting in Patients Undergoing A Thoracentesiscoosa liquorsОценок пока нет
- Inventory ManagementДокумент24 страницыInventory ManagementMohamed LaghyatiОценок пока нет
- ECPM 2021 European Congress of Perinatal MedicineДокумент1 страницаECPM 2021 European Congress of Perinatal MedicineAl DiОценок пока нет
- Code Blue Team Structures and RolesДокумент5 страницCode Blue Team Structures and RolesRSUNJAYОценок пока нет
- Scabies.: Vanessa ChelimoДокумент19 страницScabies.: Vanessa ChelimoAlvin OmondiОценок пока нет
- Tri Immunophasic Periodontal TherapyДокумент9 страницTri Immunophasic Periodontal TherapySireesha SadasivanОценок пока нет
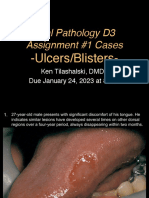
- D3 Ulcers Blisters Cases Due01242023 8amДокумент13 страницD3 Ulcers Blisters Cases Due01242023 8amLinh PhanОценок пока нет