Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- USMLE High YieldДокумент8 страницUSMLE High YieldNajia ChoudhuryОценок пока нет
- Lean GuideДокумент155 страницLean GuideSujoy Kar100% (1)
- KOICA-Yonsei Master's Program in Infectious Disease ControlДокумент28 страницKOICA-Yonsei Master's Program in Infectious Disease ControlBIDAN KSAОценок пока нет
- Answers 19521Документ845 страницAnswers 19521docerick87Оценок пока нет
- Etiology of MalocclusionДокумент28 страницEtiology of MalocclusionPriyaancaHaarsh100% (3)
- MCQPaperSept 05Документ4 страницыMCQPaperSept 05api-26291651100% (1)
- Dental Management of Medically Compromised PatientsДокумент12 страницDental Management of Medically Compromised Patientsمحمد ابوالمجدОценок пока нет
- Basic IV Therapy CalculationsДокумент35 страницBasic IV Therapy CalculationsRommel IsraelОценок пока нет
- MCQSeptember 2006 Paper IДокумент3 страницыMCQSeptember 2006 Paper Iapi-26291651100% (1)
- Cholera FinalДокумент57 страницCholera FinalBinayaОценок пока нет
- Health Promotion Prevention Plan Presentation (Capter 5)Документ42 страницыHealth Promotion Prevention Plan Presentation (Capter 5)MuniraОценок пока нет
- Biologic Width - The No Encroachment Zone: I J D AДокумент8 страницBiologic Width - The No Encroachment Zone: I J D AJinny ShawОценок пока нет
- 4 3 937Документ4 страницы4 3 937محمد ابوالمجدОценок пока нет
- Anatomy of CNSДокумент32 страницыAnatomy of CNSLeonita AguillonОценок пока нет
- Dental Cements For UseДокумент28 страницDental Cements For UseAhmed DolaОценок пока нет
- VitaminsДокумент13 страницVitaminsمحمد ابوالمجدОценок пока нет
- Publication PDFДокумент28 страницPublication PDFمحمد ابوالمجدОценок пока нет
- ChemFil Superior44Документ27 страницChemFil Superior44محمد ابوالمجدОценок пока нет
- Guidelines On Infection Control in Dental ClinicsДокумент10 страницGuidelines On Infection Control in Dental ClinicsHare RamОценок пока нет
- VitaminsДокумент13 страницVitaminsمحمد ابوالمجدОценок пока нет
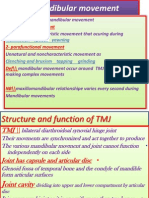
- Mandibular MovementДокумент4 страницыMandibular Movementمحمد ابوالمجدОценок пока нет
- Anatomy of CNSДокумент32 страницыAnatomy of CNSLeonita AguillonОценок пока нет
- Dental Anatomy DecksДокумент362 страницыDental Anatomy Decksapi-2629165183% (6)
- Smear LayerДокумент9 страницSmear Layerpriyanka_gedamОценок пока нет
- Publication PDFДокумент20 страницPublication PDFمحمد ابوالمجدОценок пока нет
- Mandibular MovementДокумент4 страницыMandibular Movementمحمد ابوالمجدОценок пока нет
- 1Документ15 страниц1محمد ابوالمجدОценок пока нет
- Emergency MedicineДокумент7 страницEmergency Medicineمحمد ابوالمجدОценок пока нет
- Finishing and PolishingДокумент18 страницFinishing and Polishingab0maiОценок пока нет
- Anatomy of CNSДокумент32 страницыAnatomy of CNSLeonita AguillonОценок пока нет
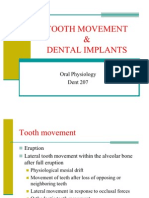
- Tooth MovementДокумент14 страницTooth Movementمحمد ابوالمجدОценок пока нет
- Behaviour Management 2Документ59 страницBehaviour Management 2Nikhil RaiОценок пока нет
- Asnan 7 RulesДокумент2 страницыAsnan 7 Rulesمحمد ابوالمجدОценок пока нет
- Serial Extraction PedoДокумент23 страницыSerial Extraction PedoSelim BaftiuОценок пока нет
- RO0111 00-00 WebberДокумент6 страницRO0111 00-00 WebberARTОценок пока нет
- DentistryДокумент71 страницаDentistryAnupama NagrajОценок пока нет
- OcclusionДокумент17 страницOcclusionمحمد ابوالمجدОценок пока нет
- MKWD Lwua Adb Package 2 AnnexesДокумент199 страницMKWD Lwua Adb Package 2 AnnexesRoland AnaumОценок пока нет
- Kindergarten q1 Week10 v2Документ33 страницыKindergarten q1 Week10 v2Aryan Angela Dela CruzОценок пока нет
- Sleep Quality and Quality of Life in FemДокумент8 страницSleep Quality and Quality of Life in FemGaith FekiОценок пока нет
- Main - Factsheet Tacrolimus OintmentДокумент4 страницыMain - Factsheet Tacrolimus OintmentSakuranbochanОценок пока нет
- Uttarakhand Dealers Data, JanviДокумент8 страницUttarakhand Dealers Data, JanviVAISHNAVI TAYALОценок пока нет
- Nutrition Counseling And Dietary InstructionДокумент5 страницNutrition Counseling And Dietary Instructionnicoleangela ubasroselloОценок пока нет
- Nutraceutical Products in India Market ReportДокумент7 страницNutraceutical Products in India Market ReportMadan Mohan Sharan SinghОценок пока нет
- Hydrogen Sulphide Safety Around RigДокумент14 страницHydrogen Sulphide Safety Around RigmohammedОценок пока нет
- KAP regarding BSE among womenДокумент30 страницKAP regarding BSE among womenrandika wijesooriyaОценок пока нет
- Breast Feeding Final ProposalДокумент16 страницBreast Feeding Final ProposalDeborah BoahemaaОценок пока нет
- Grade 7 (TLE) Week 1Документ12 страницGrade 7 (TLE) Week 1RoswlleОценок пока нет
- History Patient - Co.ukДокумент14 страницHistory Patient - Co.ukiuytrerОценок пока нет
- Conquer Your Fears and Open New Doors To Opportunity!: Vol 239 Oct 2020Документ24 страницыConquer Your Fears and Open New Doors To Opportunity!: Vol 239 Oct 2020Himanshu K SharmaОценок пока нет
- PamphletДокумент1 страницаPamphletAldenn MinotaurОценок пока нет
- THHV- 18 G10 ĐỀ NÂNG CAO TỔNG HỢP SỐ 2Документ12 страницTHHV- 18 G10 ĐỀ NÂNG CAO TỔNG HỢP SỐ 2hCby 28Оценок пока нет
- The Lord of Lost Heart PDFДокумент44 страницыThe Lord of Lost Heart PDFCouteron LaurentОценок пока нет
- PDFДокумент7 страницPDFBuloy ReggieОценок пока нет
- Autism Behaviors PresentationДокумент2 страницыAutism Behaviors Presentationapi-283422107Оценок пока нет
- ASCGULF Company: Mohammad Gousu Basha ShaikДокумент3 страницыASCGULF Company: Mohammad Gousu Basha ShaikmohammadgouseОценок пока нет
- Speech Disorders - ChildrenДокумент2 страницыSpeech Disorders - ChildrenAmanda Kenshi NurfitriОценок пока нет
- Alvarez 2015Документ18 страницAlvarez 2015Clara RodriguesОценок пока нет
- Solutions For RefugeesДокумент24 страницыSolutions For RefugeesjacquelineОценок пока нет
- 2016 3 23 9 12 47tapchi-Dhdn-So12 (97) .2015-Color-WebДокумент128 страниц2016 3 23 9 12 47tapchi-Dhdn-So12 (97) .2015-Color-WebThọ Nguyễn Văn100% (1)