Вам также может понравиться
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- MC33883Документ21 страницаMC33883Nguyen TuanОценок пока нет
- Survival Manual TipsДокумент676 страницSurvival Manual Tipssergey62100% (3)
- MCQ Question BankДокумент102 страницыMCQ Question BankdrmadaanpiyushОценок пока нет
- Fall Protection Misconceptions and Myths PDFДокумент18 страницFall Protection Misconceptions and Myths PDFsebastian9033Оценок пока нет
- DAKE Press Model 75 H - 907003Документ6 страницDAKE Press Model 75 H - 907003mark_dayОценок пока нет
- Buks IDIP Unit D Assignment, Rev. 03Документ43 страницыBuks IDIP Unit D Assignment, Rev. 03Saqib Rasool100% (5)
- MaryAnn Suicide LetterДокумент1 страницаMaryAnn Suicide LetterMaryAnne WilhelmОценок пока нет
- Dressings: Carmina Disu Diana Ray Margarita DialaДокумент15 страницDressings: Carmina Disu Diana Ray Margarita DialaNdor BariboloОценок пока нет
- Acu-Loc IIДокумент36 страницAcu-Loc IIEdnor GalvaoОценок пока нет
- Walking Shoes: Features and Fit That Keep You Moving: by Mayo Clinic StaffДокумент3 страницыWalking Shoes: Features and Fit That Keep You Moving: by Mayo Clinic StaffRaprnaОценок пока нет
- Cove Point LNG Terminal Expansion Project Risk StudyДокумент77 страницCove Point LNG Terminal Expansion Project Risk StudyjomafebaОценок пока нет
- Assignment OshaДокумент10 страницAssignment OshaAmir Psk100% (1)
- ZM-MFC1 Combo: To Ensure Safe and Easy Installation, Please Read The Following PrecautionsДокумент7 страницZM-MFC1 Combo: To Ensure Safe and Easy Installation, Please Read The Following PrecautionsnegatronnОценок пока нет
- 45 Web BK, Karate JutsuДокумент71 страница45 Web BK, Karate Jutsudiamond68100% (5)
- Nasal Fractures: HistoryДокумент9 страницNasal Fractures: Historyimran qaziОценок пока нет
- Fish Defense MechanismsДокумент13 страницFish Defense MechanismsVinu ArunagiriОценок пока нет
- Ana and Physio Lab Week 1Документ29 страницAna and Physio Lab Week 1Jobelle VergaraОценок пока нет
- Accredited Pollution Control Officer Safety Consultant Certified Applicator ISO Process OwnerДокумент32 страницыAccredited Pollution Control Officer Safety Consultant Certified Applicator ISO Process Ownerbyron eugenioОценок пока нет
- Article 14859273241Документ8 страницArticle 14859273241pokeman693Оценок пока нет
- BOSS CH1000 Manual de ServicioДокумент9 страницBOSS CH1000 Manual de Servicioelectroniclm5795Оценок пока нет
- Vertebral Column: Nicole M. Reeves, Ph.D. Department of AnatomyДокумент58 страницVertebral Column: Nicole M. Reeves, Ph.D. Department of Anatomykrishna gОценок пока нет
- Common Vocabulary Words for Grades 4-6Документ4 страницыCommon Vocabulary Words for Grades 4-6meddana19Оценок пока нет
- Knee InjuryДокумент44 страницыKnee Injuryhendi_filipus_90Оценок пока нет
- Police Shooting Leaves Student ParalyzedДокумент2 страницыPolice Shooting Leaves Student ParalyzedKarenGarcíaОценок пока нет
- Landowners Liable for Damages but Contributory Negligence Reduces AwardДокумент2 страницыLandowners Liable for Damages but Contributory Negligence Reduces AwardYunna LinnОценок пока нет
- Uefa B AssignmentДокумент23 страницыUefa B AssignmentArnelaŠabanovićОценок пока нет
- Complete DentureДокумент57 страницComplete Denturedr_ahmad_zuhdi100% (3)
- Tracheostomy CareДокумент12 страницTracheostomy CareAnusha Verghese100% (1)
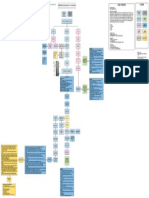
- Bone Fracture Concept MapДокумент1 страницаBone Fracture Concept MapJette Charmae OlboОценок пока нет
- Fat Embolism Syndrome: A Review of Pathophysiology, Diagnosis and ManagementДокумент26 страницFat Embolism Syndrome: A Review of Pathophysiology, Diagnosis and ManagementSuhanthi Mani100% (2)