Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Condition Formula IV Fluid Acute Gastroenteritis A. Severe Acute Malnutrition (SAM) Source: WHO?? 1. in ShockДокумент4 страницыCondition Formula IV Fluid Acute Gastroenteritis A. Severe Acute Malnutrition (SAM) Source: WHO?? 1. in ShockJohnPaulOliverosОценок пока нет
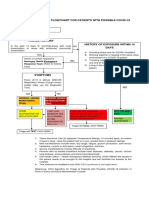
- Referral Flow Covid City HealthДокумент1 страницаReferral Flow Covid City HealthJohnPaulOliverosОценок пока нет
- Lower Gastrointestinal Bleeding: Practice EssentialsДокумент28 страницLower Gastrointestinal Bleeding: Practice EssentialsJohnPaulOliverosОценок пока нет
- Complementary and Toddler FeedingДокумент74 страницыComplementary and Toddler FeedingJohnPaulOliverosОценок пока нет
- Acute Pancreatitis ComplicationsДокумент42 страницыAcute Pancreatitis ComplicationsJohnPaulOliverosОценок пока нет
- Appointment of Oliveros John PaulДокумент3 страницыAppointment of Oliveros John PaulJohnPaulOliverosОценок пока нет
- NAC Journal Appraisal FinalДокумент32 страницыNAC Journal Appraisal FinalJohnPaulOliverosОценок пока нет
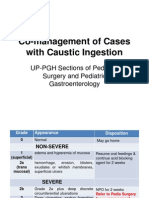
- Co-Management of Cases With Caustic Ingestion: UP-PGH Sections of Pediatric Surgery and Pediatric GastroenterologyДокумент3 страницыCo-Management of Cases With Caustic Ingestion: UP-PGH Sections of Pediatric Surgery and Pediatric GastroenterologyJohnPaulOliverosОценок пока нет
- Complementary and Toddler FeedingДокумент74 страницыComplementary and Toddler FeedingJohnPaulOliverosОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Fibromyalgia Thesis StatementДокумент7 страницFibromyalgia Thesis Statementginnysagdalenrochester100% (1)
- Short Notes: Melaka Trauma Life SupportДокумент104 страницыShort Notes: Melaka Trauma Life SupportSebastian KohОценок пока нет
- Classification of Injuries FMTДокумент30 страницClassification of Injuries FMTkhadzx100% (2)
- Nursing Thesis Sample PhilippinesДокумент6 страницNursing Thesis Sample Philippinesdngw6ed6100% (2)
- Eop AnaesДокумент26 страницEop AnaesSheera EiyraaОценок пока нет
- Date/ Time Cues Need Nursing Diagnosis Patient Outcome Planning of Intervention Implementation Evaluation Objective: - R: HypotensionДокумент5 страницDate/ Time Cues Need Nursing Diagnosis Patient Outcome Planning of Intervention Implementation Evaluation Objective: - R: HypotensionGregg AndoyОценок пока нет
- BURNДокумент101 страницаBURNLexus Nosyel100% (1)
- Drug StudyДокумент6 страницDrug StudyGeraldine Gallaron - CasipongОценок пока нет
- General Pathology MCQДокумент3 страницыGeneral Pathology MCQSooPl33% (3)
- MS CA and EN Ans KeyДокумент15 страницMS CA and EN Ans KeyAydh Dim-Mac RsclОценок пока нет
- Tanzania - SOPs For Case Management and Infection Prevention and ControlДокумент115 страницTanzania - SOPs For Case Management and Infection Prevention and ControlXuan Nguyen100% (1)
- 2013 Sepsis GuidelinesДокумент58 страниц2013 Sepsis GuidelinesMuhd Azam100% (1)
- Soap Note 5.0Документ4 страницыSoap Note 5.0Paulus IskandarОценок пока нет
- Contracted PelvisДокумент48 страницContracted Pelviskalpana shona100% (4)
- Bleeding: Mouth Nose Ear Urethra Vagina Anus SkinДокумент3 страницыBleeding: Mouth Nose Ear Urethra Vagina Anus SkinJuliet Nillo RecepcionОценок пока нет
- ShockДокумент25 страницShockSurya Mohan Jha100% (1)
- Dengue Fever by LubnaДокумент47 страницDengue Fever by LubnaDr AnilОценок пока нет
- ICU Pharmacology: Sean Forsythe M.D. Assistant Professor of MedicineДокумент52 страницыICU Pharmacology: Sean Forsythe M.D. Assistant Professor of Medicinecoolboy1990Оценок пока нет
- Medicolegal Aspects of Death InvestigationДокумент7 страницMedicolegal Aspects of Death InvestigationSuhas IngaleОценок пока нет
- CH 46 Complications of AnaesthesiaДокумент29 страницCH 46 Complications of AnaesthesiaChristian LeepoОценок пока нет
- Paper - Guidelines - Surviving Sepsis Campaign 2021Документ67 страницPaper - Guidelines - Surviving Sepsis Campaign 2021Harold JeffersonОценок пока нет
- Fect Eau 2017Документ15 страницFect Eau 2017Allison DiêgoОценок пока нет
- Shock SIRS & MODS - Lewis Flashcards - QuizletДокумент17 страницShock SIRS & MODS - Lewis Flashcards - QuizletNursyNurseОценок пока нет
- Burn Case StudyДокумент4 страницыBurn Case Studyapi-232466940Оценок пока нет
- 3rd Grading Exam (Grade 9)Документ5 страниц3rd Grading Exam (Grade 9)marynelb27100% (1)
- Shock Resident LectureДокумент38 страницShock Resident Lecturepapermate9293Оценок пока нет
- Textbook ReadingДокумент275 страницTextbook ReadingNovitasari EkaОценок пока нет
- Emergency NursingДокумент40 страницEmergency NursingJaimely ReyesОценок пока нет
- Dehydration AssessmentДокумент2 страницыDehydration AssessmentzaheerbdsОценок пока нет
- MeltdownДокумент92 страницыMeltdownMyles SamОценок пока нет