Вам также может понравиться
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Advances in Pathobiology and Management of Paget’s Disease of BoneОт EverandAdvances in Pathobiology and Management of Paget’s Disease of BoneSakamuri V. ReddyОценок пока нет
- Patho SlidesДокумент46 страницPatho Slidesapi-400411160Оценок пока нет
- Icm Course Syllabus PDFДокумент8 страницIcm Course Syllabus PDFZoya Morani100% (1)
- Medical Boards Step 2 Made Ridiculously Simple (Medicalstudyzone - Com)Документ377 страницMedical Boards Step 2 Made Ridiculously Simple (Medicalstudyzone - Com)Benyamin KhalevОценок пока нет
- Obstetrics Cases by Caroline de CostaДокумент9 страницObstetrics Cases by Caroline de CostaJeffrey HingОценок пока нет
- Pediatrics Modern Day AnalysisДокумент144 страницыPediatrics Modern Day AnalysisDaniyal AzmatОценок пока нет
- Endocrine DisordersДокумент5 страницEndocrine DisordersBilly Ray VillanuevaОценок пока нет
- Primer on the Metabolic Bone Diseases and Disorders of Mineral MetabolismОт EverandPrimer on the Metabolic Bone Diseases and Disorders of Mineral MetabolismОценок пока нет
- Disease of The Biliary TractДокумент7 страницDisease of The Biliary TractMae DoctoleroОценок пока нет
- Concept Map CholesectomyДокумент3 страницыConcept Map CholesectomyDoreen Claire100% (1)
- Drug Therapy For GI Disorders PDFДокумент5 страницDrug Therapy For GI Disorders PDFmeeraОценок пока нет
- Endocrine System - Internal MedicineДокумент39 страницEndocrine System - Internal MedicineDaanishОценок пока нет
- Diagnostic Strategy in RheumatologyДокумент25 страницDiagnostic Strategy in Rheumatologyaa031987Оценок пока нет
- Councelling and History TakingДокумент5 страницCouncelling and History TakingbashingarОценок пока нет
- Agis Mira Dewi, S.kedДокумент35 страницAgis Mira Dewi, S.kedAgiish EMdeОценок пока нет
- Synovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandSynovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- 2018 CSB520 ANSWERS Skeletal System PathologyДокумент4 страницы2018 CSB520 ANSWERS Skeletal System PathologyNathanОценок пока нет
- Respiratory AssessmentДокумент43 страницыRespiratory AssessmentLui Andrei AnilaОценок пока нет
- EV Neonatal JaundiceДокумент24 страницыEV Neonatal JaundiceAlkrenaweeSrurОценок пока нет
- Prevention of CancerДокумент2 страницыPrevention of Cancercmmc_3Оценок пока нет
- A Simple Guide to Acalculous Cholecystopathy, Diagnosis, Treatment and Related ConditionsОт EverandA Simple Guide to Acalculous Cholecystopathy, Diagnosis, Treatment and Related ConditionsОценок пока нет
- FMS 1 - Week 7 Tutorial 1 LO PDFДокумент17 страницFMS 1 - Week 7 Tutorial 1 LO PDFAprillia AlmaasОценок пока нет
- Family Medicine OSCE Dr. Rebeca HoilettДокумент20 страницFamily Medicine OSCE Dr. Rebeca HoilettFatma El FaresОценок пока нет
- Description of The Patient & Instructions To SimulatorДокумент7 страницDescription of The Patient & Instructions To SimulatorCindy WongОценок пока нет
- EBM Prognosis 2011Документ47 страницEBM Prognosis 2011Astrid AviditaОценок пока нет
- Aquifer InternalMedicine11 - 45Документ8 страницAquifer InternalMedicine11 - 45JulieОценок пока нет
- Obstetics Simplified El-MowafiДокумент515 страницObstetics Simplified El-Mowafiapi-370504650% (2)
- PD OSCE GuideДокумент19 страницPD OSCE GuideChorong ParkОценок пока нет
- BONESДокумент73 страницыBONESsafa_sabaОценок пока нет
- Common Conditions of The Lumbar SpineДокумент4 страницыCommon Conditions of The Lumbar SpineJames KОценок пока нет
- Mental Status Examination Medical StudentsДокумент23 страницыMental Status Examination Medical StudentseurocoupeОценок пока нет
- Pap SmearДокумент34 страницыPap Smearevi_ermaОценок пока нет
- Aquifer InternalMedicine09 - 55Документ7 страницAquifer InternalMedicine09 - 55JulieОценок пока нет
- Divine Intervention Episode 6 20 in 20 Pharmacology CasesДокумент21 страницаDivine Intervention Episode 6 20 in 20 Pharmacology CasesSwisskelly1Оценок пока нет
- Heart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesДокумент3 страницыHeart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesPrarthana Thiagarajan100% (3)
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsОт EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsОценок пока нет
- Divine Intervention Episode 12 Bacteria Cases AДокумент18 страницDivine Intervention Episode 12 Bacteria Cases ASwisskelly1Оценок пока нет
- Case History M.SCДокумент10 страницCase History M.SCRaksha RNОценок пока нет
- Metabolic Bone DiseaseДокумент25 страницMetabolic Bone DiseaseSavin PetersОценок пока нет
- 246 - Respiratory Pathology Pneumonia - Treatment and PreventionДокумент4 страницы246 - Respiratory Pathology Pneumonia - Treatment and PreventionPranav PunjabiОценок пока нет
- Epidemiology 2Документ15 страницEpidemiology 2Rozen Tareque HasanОценок пока нет
- BIOL 215 - CWRU Final Exam Learning GoalsДокумент32 страницыBIOL 215 - CWRU Final Exam Learning GoalsKesharaSSОценок пока нет
- HepatosplenomegalyДокумент52 страницыHepatosplenomegalySundar NatarajanОценок пока нет
- Asthma Drugs Clinical PharmacologyДокумент3 страницыAsthma Drugs Clinical PharmacologycrystalsheОценок пока нет
- Female PathologyДокумент16 страницFemale Pathologymiguel cuevasОценок пока нет
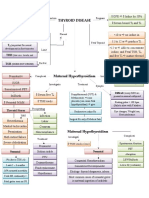
- Thyroid DiseaseДокумент1 страницаThyroid DiseaseZiyadОценок пока нет
- MusculoskeletalДокумент35 страницMusculoskeletalZeeshan SiddiquiОценок пока нет
- History & Physical ExaminationДокумент67 страницHistory & Physical ExaminationDiggi VioОценок пока нет
- Anti Viral DrugsДокумент6 страницAnti Viral DrugskakuОценок пока нет
- Hem-Onc: AnswerДокумент3 страницыHem-Onc: AnswerAman Raj KОценок пока нет
- Anatomy and Physiology of PlacentaДокумент5 страницAnatomy and Physiology of PlacentaAmuОценок пока нет
- Personal Notes Excpetional StuffДокумент352 страницыPersonal Notes Excpetional StuffYagyeshОценок пока нет
- Gastroenterology 2008Документ56 страницGastroenterology 2008Sandra Q Tran100% (1)
- 03 The Cardiorespiratory SystemДокумент24 страницы03 The Cardiorespiratory SystemDuane N Lin WertОценок пока нет
- Rheumatoid ArthritisДокумент29 страницRheumatoid ArthritisTamim IshtiaqueОценок пока нет
- Rheumatology NotesДокумент31 страницаRheumatology Noteskatherine nunnОценок пока нет
- Disorders of BonesДокумент3 страницыDisorders of BonesAnonymous 0pSLjJYОценок пока нет
- Rheumatoid Arthritis: History, Stages, Epidemiology, Pathogenesis, Diagnosis and TreatmentДокумент12 страницRheumatoid Arthritis: History, Stages, Epidemiology, Pathogenesis, Diagnosis and TreatmentAdhelaAuroraFransiskaОценок пока нет
- Rheumatoid Arthritis: Unarse, Manuel IiiДокумент23 страницыRheumatoid Arthritis: Unarse, Manuel IiiAena PortsОценок пока нет
- Case On Acute Rheumatoid ArthritisДокумент15 страницCase On Acute Rheumatoid ArthritisdeepakОценок пока нет
- Celebrex OfferДокумент13 страницCelebrex OffervjОценок пока нет
- Rheumatoid ArthritisДокумент21 страницаRheumatoid ArthritisKatrene LequiganОценок пока нет
- Wrist PainДокумент8 страницWrist PainLev KalikaОценок пока нет
- Anesthesia For Orthopedic SurgeryДокумент27 страницAnesthesia For Orthopedic Surgeryjeremy_raineyОценок пока нет
- Arthritis PDFДокумент4 страницыArthritis PDFArchana MoreyОценок пока нет
- Musculoskeletal SystemДокумент10 страницMusculoskeletal SystemPinky CuaresmaОценок пока нет
- ARTHRITISДокумент4 страницыARTHRITISJk FloresОценок пока нет
- Approach To Joint Pain-1Документ49 страницApproach To Joint Pain-1Shivangi LodhaОценок пока нет
- Medically Compromised PatientДокумент84 страницыMedically Compromised PatientShubham khandkeОценок пока нет
- Autoimmune Waterfasting PDFДокумент3 страницыAutoimmune Waterfasting PDFMihailo JankovicОценок пока нет
- Rheumatoid ArthritisДокумент4 страницыRheumatoid ArthritisFreeNursingNotes100% (1)
- Plab 2 PDFДокумент18 страницPlab 2 PDFSualeha SohailОценок пока нет
- Betnesol InformationДокумент6 страницBetnesol InformationsmazОценок пока нет
- Etiology of Rheumatoid Arthritis PDFДокумент2 страницыEtiology of Rheumatoid Arthritis PDFBoliviaОценок пока нет
- Locomotor - Hand Clinical Mark SheetДокумент7 страницLocomotor - Hand Clinical Mark SheetDrShamshad KhanОценок пока нет
- The IASP Classification of Chronic Pain For.10Документ6 страницThe IASP Classification of Chronic Pain For.10hzol83Оценок пока нет
- Rheumatoid Arthritis MEQДокумент3 страницыRheumatoid Arthritis MEQMuvenn KannanОценок пока нет
- ArthritisДокумент6 страницArthritisChristel Mariz SantellaОценок пока нет
- Careram: Tablets 25 MGДокумент6 страницCareram: Tablets 25 MGPriya Ranjan100% (1)
- A Guide To ArthritisДокумент12 страницA Guide To ArthritisConsidraCareОценок пока нет
- Contraindications of TractionДокумент3 страницыContraindications of TractionQuentene odongoОценок пока нет
- Adult Onset Stills DiseaseДокумент5 страницAdult Onset Stills Diseaseali zainalОценок пока нет
- Focused ReviewДокумент6 страницFocused ReviewGina GiammalvoОценок пока нет
- Enbrel Epar Product Information - enДокумент265 страницEnbrel Epar Product Information - enAhmed BesoОценок пока нет
- DVDGGДокумент10 страницDVDGGSilviОценок пока нет