Вам также может понравиться
- Physical Assessment of Abdomen and RectumДокумент41 страницаPhysical Assessment of Abdomen and RectumLeonilyn Dagoplo RN100% (1)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Hydrocephalus and Spina Bifida: Pathophysiology, Clinical Presentation and ManagementДокумент63 страницыHydrocephalus and Spina Bifida: Pathophysiology, Clinical Presentation and ManagementAjeng Aristiany Rahawarin100% (2)
- Anatomy and Physiology of Small and Large Intestines, Rectum and AnusДокумент24 страницыAnatomy and Physiology of Small and Large Intestines, Rectum and AnusElmer PatrickОценок пока нет
- Nutrition in Sick PatientsДокумент50 страницNutrition in Sick PatientsIbnu ZakiОценок пока нет
- Clinical Examination of The AbdomenДокумент13 страницClinical Examination of The AbdomenNur Miladiyah100% (1)
- 3 Session 3 - AbdominalExamДокумент15 страниц3 Session 3 - AbdominalExamjhk0428Оценок пока нет
- Examination of Abdominal Lump: DR Rajesh P SДокумент20 страницExamination of Abdominal Lump: DR Rajesh P SdrrajeshpsmsОценок пока нет
- The Acute AbdomenДокумент174 страницыThe Acute AbdomenHabibHusseinJasmanОценок пока нет
- PancreatitisДокумент6 страницPancreatitisMary AmaliaОценок пока нет
- Functions and anatomy of the small intestineДокумент8 страницFunctions and anatomy of the small intestineErald PaderangaОценок пока нет
- RBC Degradation & Causes of JaundiceДокумент30 страницRBC Degradation & Causes of JaundiceSubhi MishraОценок пока нет
- Acute Abdomen Causes Diagnosis TreatmentДокумент8 страницAcute Abdomen Causes Diagnosis Treatmentarum1992Оценок пока нет
- Abdominal ExaminationДокумент4 страницыAbdominal ExaminationdizhalfaОценок пока нет
- Case Sheet - Abdominal Lump in Right Lumbar RegionДокумент5 страницCase Sheet - Abdominal Lump in Right Lumbar RegionpradeepОценок пока нет
- LEC 15.1 - Abdominal HerniasДокумент37 страницLEC 15.1 - Abdominal HerniasTudor CorneaОценок пока нет
- ANDI Classification System Explains Benign Breast DisordersДокумент9 страницANDI Classification System Explains Benign Breast DisordersaprooolОценок пока нет
- Surgery UpcamДокумент11 страницSurgery UpcamArchie DuqueОценок пока нет
- INTUSSUSCEPTIONДокумент3 страницыINTUSSUSCEPTIONS GОценок пока нет
- AppendicitisДокумент36 страницAppendicitisPetro MyronovОценок пока нет
- Pancreatitis: Dr. Ahmad Aqel RN, PHD The University of Jordan 2015Документ27 страницPancreatitis: Dr. Ahmad Aqel RN, PHD The University of Jordan 2015Anonymous 5HzElnmОценок пока нет
- Chronic Suppurative Otitis MediaДокумент6 страницChronic Suppurative Otitis MediaSuhas IngaleОценок пока нет
- CHOLELITHIASISДокумент19 страницCHOLELITHIASISAnil DasОценок пока нет
- Clinical Approach To Abdominal Disorder: Kurniyanto Department of Internal MedicineДокумент68 страницClinical Approach To Abdominal Disorder: Kurniyanto Department of Internal MedicineMonica AnggiОценок пока нет
- Acute Pain Abdomen in Surgical PracticeДокумент34 страницыAcute Pain Abdomen in Surgical PracticedrakashnardeОценок пока нет
- Digestion QuizДокумент5 страницDigestion QuizneciiОценок пока нет
- Acute Abdominal Pain GuideДокумент77 страницAcute Abdominal Pain GuideGraceline Margaretha Marsintauly SianiparОценок пока нет
- Carcinoma Pancreas: Risk Factors: (A) Demographic FactorsДокумент4 страницыCarcinoma Pancreas: Risk Factors: (A) Demographic FactorsSakthi Annamalai.cОценок пока нет
- GIT Applied AnatomyДокумент62 страницыGIT Applied Anatomyueumana0% (1)
- Slides 2 - Wounds, UlcersДокумент80 страницSlides 2 - Wounds, UlcersCWT2010Оценок пока нет
- Powerpoint: Disorders of The EsophagusДокумент65 страницPowerpoint: Disorders of The Esophagusj.doe.hex_8782% (11)
- Surgical Wound ClassificationДокумент1 страницаSurgical Wound Classificationgeclear323Оценок пока нет
- Rebound Tenderness TestДокумент2 страницыRebound Tenderness TestDesya100% (1)
- 1 - Introduction To Gastroenterology (2) SlaytДокумент31 страница1 - Introduction To Gastroenterology (2) SlaytZeynep ArasОценок пока нет
- STOMAДокумент3 страницыSTOMAShafiq ZahariОценок пока нет
- StomaДокумент37 страницStomaAndryHarisОценок пока нет
- TUBERCULOSIS (Lec Community Medicine)Документ24 страницыTUBERCULOSIS (Lec Community Medicine)wanderer_1010Оценок пока нет
- Colostomy Care: Ms. Maria Aurora Acosta, RNДокумент23 страницыColostomy Care: Ms. Maria Aurora Acosta, RNFely StaAnaОценок пока нет
- Filariasis in NepalДокумент41 страницаFilariasis in NepalBinaya100% (1)
- Abdominal Aortic Aneurysmn FINAL WORDДокумент16 страницAbdominal Aortic Aneurysmn FINAL WORDErica P. ManlunasОценок пока нет
- Cardio AssessmentДокумент2 страницыCardio AssessmentMabesОценок пока нет
- Ashley Esdaile MSIII Byron Baptist MSIII Mike Pothen MS IIIДокумент77 страницAshley Esdaile MSIII Byron Baptist MSIII Mike Pothen MS IIISutapa PawarОценок пока нет
- Needle Cricothyroidotomy 2 - Hatem AlsrourДокумент32 страницыNeedle Cricothyroidotomy 2 - Hatem Alsrourhatem alsrour100% (2)
- Abnormal Chest Shape: Farjana Sharmin Junior Consultant and Outpatient InchargeДокумент12 страницAbnormal Chest Shape: Farjana Sharmin Junior Consultant and Outpatient InchargeFahim Abrar KhanОценок пока нет
- External HerniaДокумент136 страницExternal Herniasanjivdas100% (1)
- Concept of EliminationДокумент42 страницыConcept of EliminationOpen UserОценок пока нет
- Vena Cava Superior SyndromeДокумент12 страницVena Cava Superior SyndromeAgnes SetiawanОценок пока нет
- Pemeriksaan Abdomen: Dr. Suhaemi, SPPD, FinasimДокумент179 страницPemeriksaan Abdomen: Dr. Suhaemi, SPPD, FinasimiroelnafialyskaОценок пока нет
- Peptic Ulcers GuideДокумент46 страницPeptic Ulcers GuideEmmanuel MukukaОценок пока нет
- Cancer of The EsophagusДокумент31 страницаCancer of The EsophagusBiway RegalaОценок пока нет
- Incisional HerniaДокумент13 страницIncisional HerniaMaya Dewi permatasariОценок пока нет
- 6 Imaging of Acute AbdomenДокумент73 страницы6 Imaging of Acute AbdomenAliyah Tofani PawelloiОценок пока нет
- Urinary Catheterization PDFДокумент3 страницыUrinary Catheterization PDFRishabh trivediОценок пока нет
- Health Assessment ON Genito Urinary System: Submitted To: Submitted byДокумент16 страницHealth Assessment ON Genito Urinary System: Submitted To: Submitted byAnanthibalaОценок пока нет
- Mouth and oral cavity conditionsДокумент5 страницMouth and oral cavity conditionsFan EliОценок пока нет
- Surgical Drain Uses & TypesДокумент3 страницыSurgical Drain Uses & TypesYusra ShaukatОценок пока нет
- Acute Pancreatitis: Presenter:Luqman Arif Bin Ahmad Hazri Supervisor: DR DarrenДокумент25 страницAcute Pancreatitis: Presenter:Luqman Arif Bin Ahmad Hazri Supervisor: DR DarrenLuqman Arif Ahmad HazriОценок пока нет
- Gastrointestinal Anatomy and Physiology: The EssentialsОт EverandGastrointestinal Anatomy and Physiology: The EssentialsJohn F. ReinusОценок пока нет
- Lecture 20 CarcinogenesisДокумент84 страницыLecture 20 CarcinogenesisMohammad_Islam87100% (1)
- AnaemiaДокумент83 страницыAnaemiaMohammad_Islam87100% (2)
- Physiopathology SyllabusДокумент1 страницаPhysiopathology SyllabusMohammad_Islam87Оценок пока нет
- Lecture 18 Upper Digestive DiseasesДокумент63 страницыLecture 18 Upper Digestive DiseasesMohammad_Islam87Оценок пока нет
- The BreastДокумент72 страницыThe BreastMohammad_Islam87Оценок пока нет
- Plastic SurgeryДокумент11 страницPlastic SurgeryMohammad_Islam87Оценок пока нет
- Abdominal HerniaeДокумент66 страницAbdominal HerniaeMohammad_Islam87Оценок пока нет
- Curst Um Abd EnglДокумент10 страницCurst Um Abd EnglMohammad_Islam87Оценок пока нет
- Lecture 17 DiabetesДокумент51 страницаLecture 17 DiabetesMohammad_Islam87Оценок пока нет
- Pharmacology Lecture 12-5-2009, OpiodsДокумент18 страницPharmacology Lecture 12-5-2009, OpiodsMohammad_Islam87Оценок пока нет
- The LymphomasДокумент46 страницThe LymphomasMohammad_Islam87Оценок пока нет
- Liver Curs 2009Документ215 страницLiver Curs 2009Mohammad_Islam87Оценок пока нет
- Borcane TumorДокумент14 страницBorcane TumorMohammad_Islam87Оценок пока нет
- Morphopathology SET 16 Pathologies of The Gastrointestinal TractДокумент29 страницMorphopathology SET 16 Pathologies of The Gastrointestinal TractMohammad_Islam87Оценок пока нет
- Morphopathology SET 15 Renal Pathologies: by Qamar AhmadДокумент25 страницMorphopathology SET 15 Renal Pathologies: by Qamar AhmadMohammad_Islam87Оценок пока нет
- Morphopathology Macroscopy (Romanian-Batch)Документ187 страницMorphopathology Macroscopy (Romanian-Batch)Mohammad_Islam87100% (1)
- Pharmacology Lecture 19-5-2009, NSAIDSДокумент19 страницPharmacology Lecture 19-5-2009, NSAIDSMohammad_Islam87Оценок пока нет
- Morphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadДокумент19 страницMorphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadMohammad_Islam87Оценок пока нет
- Morphopathology SET14 Respiratory Pathologies: by Qamar AhmadДокумент18 страницMorphopathology SET14 Respiratory Pathologies: by Qamar AhmadMohammad_Islam87Оценок пока нет
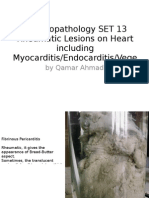
- Morphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeДокумент25 страницMorphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeMohammad_Islam87Оценок пока нет
- Borcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarДокумент7 страницBorcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Оценок пока нет
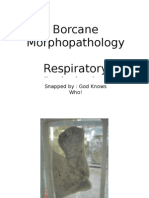
- Borcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarДокумент11 страницBorcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Оценок пока нет
- Pharmacology Lecture 5-5-2009Документ15 страницPharmacology Lecture 5-5-2009Mohammad_Islam87Оценок пока нет
- Pharmacology Lecture Diuretic Agents (High Quality)Документ15 страницPharmacology Lecture Diuretic Agents (High Quality)Mohammad_Islam87Оценок пока нет
- Borcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarДокумент7 страницBorcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87100% (1)
- Workshop 20Документ2 страницыWorkshop 20Mohammad_Islam87Оценок пока нет
- Workshop 19Документ3 страницыWorkshop 19Mohammad_Islam87Оценок пока нет
- ?#ry%oefr: - J4 @,8/ MryДокумент15 страниц?#ry%oefr: - J4 @,8/ MryMohammad_Islam87Оценок пока нет
- Engl BUN - EditДокумент167 страницEngl BUN - EditMohammad_Islam87Оценок пока нет
- Conditions Presenting With Abdominal PainДокумент69 страницConditions Presenting With Abdominal PainaimanОценок пока нет
- Psy RatsДокумент11 страницPsy RatsRavi KumarОценок пока нет
- Medical Surgical ReviewerДокумент6 страницMedical Surgical ReviewerCatherine Kaye PerezОценок пока нет
- Cu 31924071194728Документ428 страницCu 31924071194728Sahariel100% (1)
- Maximize Your Body PotentialДокумент5 страницMaximize Your Body PotentialwashawОценок пока нет
- Mental Status ExamДокумент10 страницMental Status ExamSrini VoruОценок пока нет
- Heart Healthy Diet DiscussionДокумент3 страницыHeart Healthy Diet DiscussionBilkil GuardiansОценок пока нет
- ANNB Timeline v8.2Документ1 страницаANNB Timeline v8.2Mihai BicaОценок пока нет
- All Therapy 200 RATOS 2010Документ284 страницыAll Therapy 200 RATOS 2010Bhargavi SunkiОценок пока нет
- Case Study 2 - PancreatitisДокумент1 страницаCase Study 2 - Pancreatitisapi-389612279Оценок пока нет
- Mock Board 1Документ16 страницMock Board 1russeldabon24Оценок пока нет
- Annotated BibliographyДокумент4 страницыAnnotated Bibliographyapi-271944428Оценок пока нет
- Threats of Vector-Borne Zoonotic Disease in Europe: Dogs, Drosophilids, and Oriental Eye WormДокумент3 страницыThreats of Vector-Borne Zoonotic Disease in Europe: Dogs, Drosophilids, and Oriental Eye WormGustavo AndresОценок пока нет
- Obstetric EmbolismДокумент81 страницаObstetric Embolismmiss_izzniОценок пока нет
- Roseola PDFДокумент1 страницаRoseola PDFLili PredescuОценок пока нет
- Anatomy and Physiology (Status Epilepticus)Документ3 страницыAnatomy and Physiology (Status Epilepticus)Marvin John Labiano33% (3)
- Antiepileptic Drugs 2019 Elearning PDFДокумент39 страницAntiepileptic Drugs 2019 Elearning PDFMalvika BabuОценок пока нет
- Form 10-I Certificate for Medical DeductionДокумент2 страницыForm 10-I Certificate for Medical DeductionTempuserОценок пока нет
- Obstectric and Gynaecology 3 Year 6 Batch: MCQ (Obe - One Best Answer)Документ5 страницObstectric and Gynaecology 3 Year 6 Batch: MCQ (Obe - One Best Answer)Zeke EdgeОценок пока нет
- Ewen Vs National Hockey LeagueДокумент80 страницEwen Vs National Hockey LeagueAnonymous LRPtKqjQSyОценок пока нет
- Healthy Habits PPT Grade 11Документ20 страницHealthy Habits PPT Grade 11Alex ValdecañasОценок пока нет
- Erik Ravelo 10-11 AssignmentДокумент9 страницErik Ravelo 10-11 Assignmentapi-238741224Оценок пока нет
- AB PSY PRE-BOARD 2 (June 17, 2023)Документ8 страницAB PSY PRE-BOARD 2 (June 17, 2023)sdfghОценок пока нет
- Illuminating The Mother of Qi: Intravenous and Transcutaneous Laser Blood Irradiation As Well As ExtracorporealДокумент0 страницIlluminating The Mother of Qi: Intravenous and Transcutaneous Laser Blood Irradiation As Well As ExtracorporealfghjhgfОценок пока нет
- IB Biology Option D - HL NotesДокумент33 страницыIB Biology Option D - HL NotesTheIBGeoKid75% (4)
- Psychosomatic Pain: Ertuğrul AllahverdiДокумент20 страницPsychosomatic Pain: Ertuğrul AllahverdidiasОценок пока нет
- QuestionДокумент63 страницыQuestionEdwin JohnОценок пока нет
- DAFTAR PUSTAKA Microbiology ReferencesДокумент4 страницыDAFTAR PUSTAKA Microbiology ReferencesTogu NaiposposОценок пока нет
- Acute Respiratory Distress in ChildrenДокумент25 страницAcute Respiratory Distress in Childrensai ram100% (1)
- Edward Shorter - Max Fink - The Madness of Fear - A History of Catatonia (2018, Oxford University Press) - Libgen - LiДокумент225 страницEdward Shorter - Max Fink - The Madness of Fear - A History of Catatonia (2018, Oxford University Press) - Libgen - LiCristel YadiraОценок пока нет
- Case Report of BGTДокумент5 страницCase Report of BGTZainub A KhanОценок пока нет