Вам также может понравиться
- Guillane Barre SyndromeДокумент8 страницGuillane Barre SyndromeyasiraОценок пока нет
- Guillain Barre SyndromeДокумент23 страницыGuillain Barre Syndromeleenie_goni100% (1)
- Hypertensive EncephalopathyДокумент7 страницHypertensive Encephalopathymery indrawatiОценок пока нет
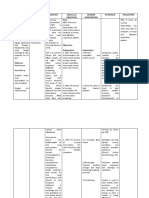
- Cues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalДокумент4 страницыCues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalMonica Angelique SalayoОценок пока нет
- Introduction CASE STUDYДокумент3 страницыIntroduction CASE STUDYDavid CalaloОценок пока нет
- A Case Study On Septic ShockДокумент51 страницаA Case Study On Septic ShockKeThSantibanОценок пока нет
- Case Report No1Документ9 страницCase Report No1Menn PetchuayОценок пока нет
- NCPДокумент6 страницNCPBon BonОценок пока нет
- Lab 5 Diabetes InsipidusДокумент6 страницLab 5 Diabetes InsipidusLisa EkapratiwiОценок пока нет
- Hassan Tonic - Clonic SeizureДокумент12 страницHassan Tonic - Clonic SeizureHassan.shehri100% (1)
- Iabetic Europathy: DR Saumya H Mittal Neurologist Sharda Hospital & Health CityДокумент39 страницIabetic Europathy: DR Saumya H Mittal Neurologist Sharda Hospital & Health CityGhea SugihartiОценок пока нет
- Pathophysiology: Bipolar DisorderДокумент3 страницыPathophysiology: Bipolar DisorderPae EdejerОценок пока нет
- Anatomy and Physiology DengueДокумент5 страницAnatomy and Physiology Denguenva226Оценок пока нет
- VSIM Clinical Worksheet 07.16.2020Документ6 страницVSIM Clinical Worksheet 07.16.2020Jackie GriffisОценок пока нет
- MyelomeningoceleДокумент7 страницMyelomeningocelemavefigОценок пока нет
- A Drug Study On FansidarДокумент7 страницA Drug Study On FansidarCasey EmellanoОценок пока нет
- Case Report GBSДокумент31 страницаCase Report GBSAde MayashitaОценок пока нет
- History: Symptoms Associated With Specific Viral InfectionsДокумент12 страницHistory: Symptoms Associated With Specific Viral InfectionsFatima Love Ariate-ArcasetasОценок пока нет
- Hiv Case StudyДокумент2 страницыHiv Case Studyapi-485814878Оценок пока нет
- 18 Measles (Rubeola)Документ12 страниц18 Measles (Rubeola)Sheryl ElitaОценок пока нет
- BSN4D-SG2 DM Type2Документ201 страницаBSN4D-SG2 DM Type2Charisse CaydanОценок пока нет
- Drug and NCPДокумент15 страницDrug and NCPgeelawlietОценок пока нет
- Undifferentiated SchizophreniaДокумент7 страницUndifferentiated SchizophreniaLovely San SebastianОценок пока нет
- 6 Nursing Care Plan 1Документ2 страницы6 Nursing Care Plan 1Denise Louise PoОценок пока нет
- MeaslesДокумент32 страницыMeaslesYum C100% (2)
- Grand Case Presentation (MI, COPD and BPH)Документ80 страницGrand Case Presentation (MI, COPD and BPH)Sarah Lim100% (2)
- Surgical InstrumentДокумент5 страницSurgical Instrumentria_soriano_2100% (1)
- Cu 3 Week 3Документ3 страницыCu 3 Week 3Maica LectanaОценок пока нет
- Rabies: Ragina AguilaДокумент55 страницRabies: Ragina AguilaCharles Lester AdalimОценок пока нет
- Cholecystectomy (: Laparoscopic GallstonesДокумент4 страницыCholecystectomy (: Laparoscopic GallstonesAlexia BatungbacalОценок пока нет
- What Is Stroke?: BY: Luis Alberto Sanchez Hernandez Physical TherapistДокумент12 страницWhat Is Stroke?: BY: Luis Alberto Sanchez Hernandez Physical TherapistLidiaAMonroyRОценок пока нет
- Study Questions: Burn InjuriesДокумент2 страницыStudy Questions: Burn InjuriesBELTRAN, JEANNE MAURICEОценок пока нет
- Tuberculous MeningitisДокумент11 страницTuberculous MeningitiszuhriОценок пока нет
- Tuberculous MeningitisДокумент23 страницыTuberculous MeningitisAsma KhmОценок пока нет
- InTech-Diabetic Foot and GangreneДокумент25 страницInTech-Diabetic Foot and GangrenePutu Reza Sandhya PratamaОценок пока нет
- ScriptДокумент2 страницыScriptKeith AquinoОценок пока нет
- Hemorrhagic Cerebro Vascular DiseaseДокумент37 страницHemorrhagic Cerebro Vascular Diseasejbvaldez100% (1)
- Case Presentation (Final)Документ35 страницCase Presentation (Final)Denie BoyonasОценок пока нет
- Definition of PneumoniaДокумент4 страницыDefinition of PneumoniaEmylia Ananda PutriОценок пока нет
- Amoebiasis Is An Infection in The Bowel, Particularly The Colon, Characterized byДокумент8 страницAmoebiasis Is An Infection in The Bowel, Particularly The Colon, Characterized byJamie JunioОценок пока нет
- (Olfu) Pediatrics Case Study: Post Streptococcal Glomerulo Nephritis (PSGN)Документ20 страниц(Olfu) Pediatrics Case Study: Post Streptococcal Glomerulo Nephritis (PSGN)MikaCasimiroBalunanОценок пока нет
- Schizophrenia ParanoidДокумент129 страницSchizophrenia ParanoidhjhjhjkjkОценок пока нет
- Guillain-Barré Syndrome: A Clinical Study of Twenty ChildrenДокумент4 страницыGuillain-Barré Syndrome: A Clinical Study of Twenty ChildrenNur Asmi RachmawatiОценок пока нет
- PYOMYOSITISДокумент6 страницPYOMYOSITISChristine CoridoОценок пока нет
- HemophiliaДокумент4 страницыHemophiliaMechelle ChenОценок пока нет
- Patient Case Presentation Rabies 28EM29Документ36 страницPatient Case Presentation Rabies 28EM29Viorica Gavriliță100% (1)
- Seizure DisorderДокумент4 страницыSeizure DisorderJohanna ChavezОценок пока нет
- Assessment of Immune FunctionДокумент3 страницыAssessment of Immune Functionhalloween candyОценок пока нет
- Guillain - Barre Syndrome FINALДокумент25 страницGuillain - Barre Syndrome FINALEunji KimОценок пока нет
- Quiz LeukemiaДокумент4 страницыQuiz LeukemiaHanna La MadridОценок пока нет
- Au Di Minor Case Study Myasthenia GravisДокумент17 страницAu Di Minor Case Study Myasthenia Gravisapi-301816885Оценок пока нет
- Meniere's Disease - Case StudyДокумент3 страницыMeniere's Disease - Case StudyZORANASNОценок пока нет
- 51 100Документ18 страниц51 100Jaessa Feliciano100% (1)
- Case Presentation About Spinal Shock SyndromeДокумент56 страницCase Presentation About Spinal Shock SyndromeAstral_edge010100% (1)
- Askep Pasien Yang Mengalami Guillain-Barré Syndrome: Maridi M. DirdjoДокумент14 страницAskep Pasien Yang Mengalami Guillain-Barré Syndrome: Maridi M. DirdjoPalupi Setyo HapsariОценок пока нет
- Mounika G1Документ8 страницMounika G1pandem soniyaОценок пока нет
- Guillain-Barre Syndrome: Presented by DR - Ruma Dey Dept. of KayachikitsaДокумент33 страницыGuillain-Barre Syndrome: Presented by DR - Ruma Dey Dept. of KayachikitsaSushanta DasОценок пока нет
- Neuromuscular DiseasesДокумент85 страницNeuromuscular DiseasesAaron James GrayОценок пока нет
- Guillain-Barré Syndrome (GBS)Документ17 страницGuillain-Barré Syndrome (GBS)Desima Tamara sinuratОценок пока нет
- Gullain Barre SyndromeДокумент33 страницыGullain Barre SyndromeNor Ubudiah SetiОценок пока нет
- Placenta PreviaДокумент10 страницPlacenta PreviaAgnes NesiaОценок пока нет
- Acne Vulgaris: Cynthia Salinas, M.D. PGY-3 Patient Conference February 2, 2005Документ29 страницAcne Vulgaris: Cynthia Salinas, M.D. PGY-3 Patient Conference February 2, 2005Agnes NesiaОценок пока нет
- Blount's Disease: Unit 6 Assignment October 11, 2011 Kathryn Bonvillian Jillianne HartДокумент20 страницBlount's Disease: Unit 6 Assignment October 11, 2011 Kathryn Bonvillian Jillianne HartAgnes NesiaОценок пока нет
- Acne Vulgaris: Cynthia Salinas, M.D. PGY-3 Patient Conference February 2, 2005Документ29 страницAcne Vulgaris: Cynthia Salinas, M.D. PGY-3 Patient Conference February 2, 2005Agnes NesiaОценок пока нет
- Credit Functions - Developmental and Promotional Functions - Supervisory FunctionsДокумент32 страницыCredit Functions - Developmental and Promotional Functions - Supervisory FunctionscrajkumarsinghОценок пока нет
- MBSR Practice ManualДокумент32 страницыMBSR Practice Manualkika100% (1)
- Phobia ListsДокумент5 страницPhobia Listskatts4uОценок пока нет
- Dissection Guide On The Frog Muscular SystemДокумент6 страницDissection Guide On The Frog Muscular SystemNeileene Joy Simeon DomingoОценок пока нет
- Protochordata FIXДокумент33 страницыProtochordata FIXSylvia AnggraeniОценок пока нет
- CucigДокумент4 страницыCucigBeto AravenaОценок пока нет
- Animal Classification Chapter Assessment Science and Technology Part 2 STD 10th English Medium1572016893Документ2 страницыAnimal Classification Chapter Assessment Science and Technology Part 2 STD 10th English Medium1572016893Chinmay KotkarОценок пока нет
- Polar Bear (Report Text)Документ14 страницPolar Bear (Report Text)Adeb Wahyu100% (1)
- Huntingtons 1Документ9 страницHuntingtons 1api-319386998Оценок пока нет
- 0610 s17 QP 31Документ24 страницы0610 s17 QP 31BioScMentor-1Оценок пока нет
- Cytoskeletal AbnormalitiesДокумент80 страницCytoskeletal Abnormalitieschinnnababu89% (9)
- Zoo Tycoon: Complete Collection - Cheats and Codes: Easy MoneyДокумент3 страницыZoo Tycoon: Complete Collection - Cheats and Codes: Easy MoneypianochecheОценок пока нет
- Perbedaan Papila Dan Folikel Pada MataДокумент2 страницыPerbedaan Papila Dan Folikel Pada MataMuhammad Agus Nashir100% (1)
- Traducere in Engleza Site Spring Dental Mihaela VelcuДокумент11 страницTraducere in Engleza Site Spring Dental Mihaela VelcuFlorin Cornel VelcuОценок пока нет
- RSM Osce Sheets 2009Документ26 страницRSM Osce Sheets 2009Derek Ho100% (2)
- Anorectal MalformationДокумент28 страницAnorectal MalformationJaya Prabha33% (3)
- اللقاحاتДокумент4 страницыاللقاحاتيمني مطنوخОценок пока нет
- Comparative Anatomy of The Horse, Ox, and Dog-The Brain and Associated VesselsДокумент11 страницComparative Anatomy of The Horse, Ox, and Dog-The Brain and Associated VesselsmichiparisОценок пока нет
- A Health Education On PneumoniaДокумент3 страницыA Health Education On PneumoniaJoshuaОценок пока нет
- Área Superficial y Volumen 3 2Документ3 страницыÁrea Superficial y Volumen 3 2Felipe Carrera (Student)Оценок пока нет
- Jumc Lab Technician Provisional Answer KeyДокумент23 страницыJumc Lab Technician Provisional Answer KeyKishor VaghaniОценок пока нет
- Introduction To Medical TerminologyДокумент8 страницIntroduction To Medical Terminologysafi_bhutto100% (2)
- Sensory Play Activities Kids Will LoveДокумент5 страницSensory Play Activities Kids Will LoveGoh KokMingОценок пока нет
- Gastro Lab ManualДокумент28 страницGastro Lab ManualYeniОценок пока нет
- Pneumonia Concept Map - KPoindexterДокумент1 страницаPneumonia Concept Map - KPoindexterKatie_Poindext_5154100% (2)
- PDF 5000 Most Common Wordspdf DDДокумент41 страницаPDF 5000 Most Common Wordspdf DDYoussef EL IdrissiiОценок пока нет
- 101 DalmatiansДокумент2 страницы101 Dalmatiansmacarong_uongsuatuoiОценок пока нет
- My Narrative ReportДокумент3 страницыMy Narrative ReportDave DoncilloОценок пока нет
- Histology of Heart and Vessels - ANAT3888 - 2023Документ41 страницаHistology of Heart and Vessels - ANAT3888 - 2023RachaelОценок пока нет
- Journal IPSG 5Документ7 страницJournal IPSG 5marissa ulkhairОценок пока нет