Вам также может понравиться
- Pathology InflammationДокумент111 страницPathology InflammationAlyssa ArroyoОценок пока нет
- Acute InflammationДокумент55 страницAcute InflammationMohammad_Islam8790% (10)
- Breast Self ExaminationДокумент13 страницBreast Self ExaminationChanDa DasОценок пока нет
- Body Fluids-1: Fluid Compartments of The Body Fluid and Electrolyte CompositionДокумент33 страницыBody Fluids-1: Fluid Compartments of The Body Fluid and Electrolyte CompositionMan LingОценок пока нет
- Sigmoid Volvulus: Rashid Swed S. (Md4) Mwanyingili John A. (Md3)Документ46 страницSigmoid Volvulus: Rashid Swed S. (Md4) Mwanyingili John A. (Md3)Amani Twaha MsemakweliОценок пока нет
- Leprosy PDFДокумент19 страницLeprosy PDFsteffiecruz06Оценок пока нет
- Comm Med McqsДокумент25 страницComm Med McqsanojanОценок пока нет
- ENCEPHALITISДокумент37 страницENCEPHALITISNida NaazОценок пока нет
- Chronic SinusitisДокумент30 страницChronic SinusitisAbdiqani MahdiОценок пока нет
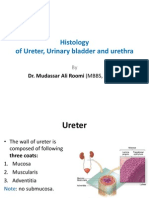
- Histology of Ureter, Urinary Bladder and Urethra by Dr. RoomiДокумент20 страницHistology of Ureter, Urinary Bladder and Urethra by Dr. RoomiMudassar Roomi100% (4)
- BRONCHOPNEUMONIA: AN OVERVIEWДокумент18 страницBRONCHOPNEUMONIA: AN OVERVIEWMANEESH MANIОценок пока нет
- HAEMORRHAGE Seminar-IДокумент25 страницHAEMORRHAGE Seminar-ISimran Josan100% (1)
- Managing patient comfort and safety devicesДокумент296 страницManaging patient comfort and safety devicesCHALIE MEQUОценок пока нет
- Bone Formation & GrowthДокумент3 страницыBone Formation & GrowtherinОценок пока нет
- Inflammation and Wound Healing Guide: Causes, Signs, Types, and StagesДокумент46 страницInflammation and Wound Healing Guide: Causes, Signs, Types, and StagesVijetha RaiОценок пока нет
- Anatomy of DuodenumДокумент23 страницыAnatomy of DuodenumEngki AdityaОценок пока нет
- CELL INJURY, DEATH, AND ADAPTATION: CAUSES AND MECHANISMSДокумент46 страницCELL INJURY, DEATH, AND ADAPTATION: CAUSES AND MECHANISMSeri_tariganОценок пока нет
- UnconsciousnessДокумент16 страницUnconsciousnessAkhilesh BabuОценок пока нет
- PoliomyelitisДокумент43 страницыPoliomyelitisGurpreet KaurОценок пока нет
- Health Assessment MCQs QuizДокумент6 страницHealth Assessment MCQs QuizAddisu Sertsu100% (1)
- Wound Healing Process ExplainedДокумент5 страницWound Healing Process ExplainedMd Ahsanuzzaman PinkuОценок пока нет
- Anatomy and Physiology of HeartДокумент5 страницAnatomy and Physiology of HeartAmit MartinОценок пока нет
- Respiratory System DisordersДокумент9 страницRespiratory System Disordersasop06Оценок пока нет
- Pathology Methods and Techniques GuideДокумент15 страницPathology Methods and Techniques GuideKiran100% (1)
- ITP (Idiopathic Thrombocytopenic Purpura)Документ20 страницITP (Idiopathic Thrombocytopenic Purpura)Iqra NaseemОценок пока нет
- MCQ On NeurologyДокумент2 страницыMCQ On NeurologynamsoОценок пока нет
- New PPT For HepatitisДокумент88 страницNew PPT For HepatitisPriya100% (1)
- Kenya National Immunization Policy Guidelines Version SignedДокумент100 страницKenya National Immunization Policy Guidelines Version SignedHarriet Temba100% (1)
- Nursing Care PneumoniaДокумент26 страницNursing Care PneumoniaIsaac Kipkemoi100% (1)
- SHOCKДокумент35 страницSHOCKsami azadОценок пока нет
- Sociology and NursingДокумент4 страницыSociology and NursingMushtaq Ali100% (1)
- MCB204 Wound Healing AssignmentДокумент5 страницMCB204 Wound Healing AssignmentShamaОценок пока нет
- Community Health One LinersДокумент30 страницCommunity Health One LinersRatan YadavОценок пока нет
- Deviated Nasal Septum: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarДокумент13 страницDeviated Nasal Septum: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarSuhas IngaleОценок пока нет
- ANATOMY and PHYSIOLOGY of CHRONIC OTITIS MEDIA-GCS Sa MED - ANNEX-maam ValezaДокумент36 страницANATOMY and PHYSIOLOGY of CHRONIC OTITIS MEDIA-GCS Sa MED - ANNEX-maam ValezaBonieve Pitogo NoblezadaОценок пока нет
- Anatomy - Multiple Choice - 10 Questions: Mark Each Statement Either True/ FalseДокумент2 страницыAnatomy - Multiple Choice - 10 Questions: Mark Each Statement Either True/ FalseanojanОценок пока нет
- Checklist For PhototherapyДокумент6 страницChecklist For PhototherapyAdolf HitlerОценок пока нет
- CVP MonitoringДокумент24 страницыCVP MonitoringChoji Heiwajima100% (1)
- Filariasis in NepalДокумент41 страницаFilariasis in NepalBinaya100% (1)
- NephritisДокумент21 страницаNephritisruchikaОценок пока нет
- SummaryДокумент4 страницыSummaryDyam MitchОценок пока нет
- Hypersensitivity ReactionsДокумент25 страницHypersensitivity Reactionsbpt2100% (3)
- Lung Abscess Causes and TreatmentДокумент28 страницLung Abscess Causes and TreatmentBobet ReñaОценок пока нет
- Assessment of Respiratory SystemДокумент34 страницыAssessment of Respiratory SystemKristal Jade Yanto Esquillo100% (1)
- Understanding HaemorrhageДокумент23 страницыUnderstanding HaemorrhageAvneet MaanОценок пока нет
- Bone Marrow ChecklistДокумент2 страницыBone Marrow ChecklistHasyim SuparlanОценок пока нет
- Respiratory System - Anatomy & PhysiologyДокумент24 страницыRespiratory System - Anatomy & PhysiologySarthak ShahОценок пока нет
- Metabolic Response To InjuryДокумент55 страницMetabolic Response To InjuryMuhammad NaveedОценок пока нет
- Seminar 2 Endocrine DisordersДокумент44 страницыSeminar 2 Endocrine DisordersSuganthi ParthibanОценок пока нет
- Lower Respiratory Tract InfectionДокумент21 страницаLower Respiratory Tract InfectionJohn Vincent Dy OcampoОценок пока нет
- Epidemiological TriadДокумент14 страницEpidemiological TriadmanjulaОценок пока нет
- MUSCLE PHYSIOLOGY: AN OVERVIEWДокумент50 страницMUSCLE PHYSIOLOGY: AN OVERVIEWJoyce Adjei-boateng100% (1)
- Childhood Lymphoma Types, Stages, and TreatmentДокумент42 страницыChildhood Lymphoma Types, Stages, and TreatmentPriyaОценок пока нет
- Understanding HemiplegiaДокумент12 страницUnderstanding Hemiplegiagliffinz100% (1)
- History and Physical Assessment of the Integumentary SystemДокумент84 страницыHistory and Physical Assessment of the Integumentary SystemNilakshi Barik MandalОценок пока нет
- Pulse Oximetry v2Документ15 страницPulse Oximetry v2sars_86Оценок пока нет
- 11 - Professional SecrecyДокумент10 страниц11 - Professional SecrecyTrishenth Fonseka100% (1)
- Management of Tuberculosis: A guide for clinicians (eBook edition)От EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Оценок пока нет
- WBC DisordersДокумент32 страницыWBC Disordersbpt295% (19)
- Valvular Heart DiseasesДокумент29 страницValvular Heart Diseasesbpt2Оценок пока нет
- Undernutrition & ObesityДокумент17 страницUndernutrition & Obesitybpt2Оценок пока нет
- OsteomyelitisДокумент13 страницOsteomyelitisbpt2100% (2)
- My Op at HiesДокумент22 страницыMy Op at Hiesbpt2Оценок пока нет
- Tumors of The Nervous SystemДокумент12 страницTumors of The Nervous Systembpt20% (1)
- Teaching ScheduleДокумент2 страницыTeaching Schedulebpt2Оценок пока нет
- Peripheral Nerve DisordersДокумент33 страницыPeripheral Nerve Disordersbpt2Оценок пока нет
- Septic ArthritisДокумент12 страницSeptic Arthritisbpt2Оценок пока нет
- RepairДокумент32 страницыRepairbpt2Оценок пока нет
- RBC DisordersДокумент27 страницRBC Disordersbpt2100% (1)
- OpdДокумент29 страницOpdbpt2100% (1)
- Learning Objectives For 3rd March 2009Документ1 страницаLearning Objectives For 3rd March 2009bpt2Оценок пока нет
- Muscle InjuryДокумент13 страницMuscle Injurybpt2Оценок пока нет
- NeoplasiaДокумент21 страницаNeoplasiabpt2Оценок пока нет
- Hemodynamic DisordersДокумент20 страницHemodynamic Disordersbpt2Оценок пока нет
- Muscular DystrophiesДокумент13 страницMuscular Dystrophiesbpt2Оценок пока нет
- Metabolic Bone DisordersДокумент24 страницыMetabolic Bone Disordersbpt20% (1)
- Hypersensitivity ReactionsДокумент25 страницHypersensitivity Reactionsbpt2100% (3)
- Disorders of The Hepatobiliary System: Dr. Mehzabin AhmedДокумент27 страницDisorders of The Hepatobiliary System: Dr. Mehzabin Ahmedbpt2100% (1)
- Ischemic Heart DiseaseДокумент20 страницIschemic Heart Diseasebpt2Оценок пока нет
- Lung Infections-17th March 2009Документ1 страницаLung Infections-17th March 2009bpt2Оценок пока нет
- Injury To Nerves Lecture 2BPT Oct 2007Документ17 страницInjury To Nerves Lecture 2BPT Oct 2007bpt2Оценок пока нет
- Pneumocystis Carinii Pneumonia-Bilateral, Fluffy Pulmonary Infiltrates, Prominent in The Hilum and Base of The LungsДокумент17 страницPneumocystis Carinii Pneumonia-Bilateral, Fluffy Pulmonary Infiltrates, Prominent in The Hilum and Base of The Lungsbpt2Оценок пока нет
- Injuries Due To Extremes of Temperature and PressureДокумент12 страницInjuries Due To Extremes of Temperature and Pressurebpt2Оценок пока нет
- GIT DisordersДокумент28 страницGIT Disordersbpt2100% (1)
- Immunodeficiency DisordersДокумент8 страницImmunodeficiency Disordersbpt2Оценок пока нет
- Gene DefectsДокумент30 страницGene Defectsbpt2Оценок пока нет
- Hemodynaic Disorders - IIДокумент16 страницHemodynaic Disorders - IIbpt2Оценок пока нет
- Fracture HealingДокумент16 страницFracture Healingbpt2100% (1)
- Biology 9th Solving A Biological ProblemДокумент5 страницBiology 9th Solving A Biological Problemmhussainshigri786Оценок пока нет
- CEFSK1 Aspergillus (Eng, Ital, Span, Ger, Fre) KD 12-13Документ3 страницыCEFSK1 Aspergillus (Eng, Ital, Span, Ger, Fre) KD 12-13fcincilaОценок пока нет
- Bullous Diseases Classification and TreatmentsДокумент19 страницBullous Diseases Classification and TreatmentsVicky Ilda ViantiniОценок пока нет
- 14 HF-Limfoma GI TractДокумент27 страниц14 HF-Limfoma GI TractNur akilaОценок пока нет
- Staphylococcus (Staphylococcus Aureus, Staphylococcus Epidermidis, and Staphylococcus Saprophyticus)Документ27 страницStaphylococcus (Staphylococcus Aureus, Staphylococcus Epidermidis, and Staphylococcus Saprophyticus)drparachuru100% (1)
- CytomegalovirusДокумент7 страницCytomegalovirusМохаммед МахОценок пока нет
- NO. TGL Nama RM: JANUARI 2014Документ481 страницаNO. TGL Nama RM: JANUARI 2014DewieqJunexОценок пока нет
- Annotated BibliographyДокумент7 страницAnnotated Bibliographyapi-202202577Оценок пока нет
- Microbiology Lecture - 20 Enterovirus & HepatitisДокумент64 страницыMicrobiology Lecture - 20 Enterovirus & HepatitisChris Queiklin100% (1)
- Covid-19 SOP Flow Chart for Manufacturing CompanyДокумент6 страницCovid-19 SOP Flow Chart for Manufacturing CompanynorfilzahОценок пока нет
- FILIRIASISДокумент25 страницFILIRIASISJoy Gao-ayОценок пока нет
- Pathophysiology of Leptospirosis and Dengue FeverДокумент5 страницPathophysiology of Leptospirosis and Dengue FeverKenneth Lagman100% (1)
- Pediatric Soap NoteДокумент4 страницыPediatric Soap NoteAfinaMuthi50% (2)
- Kuliah Biokimia-Imunokimia FK UNDIPДокумент19 страницKuliah Biokimia-Imunokimia FK UNDIPPutri HapsariОценок пока нет
- Barangay Monthly Inventory of Vaccinated PopulationДокумент2 страницыBarangay Monthly Inventory of Vaccinated PopulationGenzo TaniaОценок пока нет
- Oral Medicine - Update For The Dental Practitioner Lumps and SwellingsДокумент9 страницOral Medicine - Update For The Dental Practitioner Lumps and SwellingsGowriОценок пока нет
- Reference: Harmening, D.M. (2012) - Modern Blood Banking & Transfusion Practices. 6 Ed. Pg. 123. F.A. Davis CompanyДокумент2 страницыReference: Harmening, D.M. (2012) - Modern Blood Banking & Transfusion Practices. 6 Ed. Pg. 123. F.A. Davis CompanyMARC AIVIN BEATOОценок пока нет
- Respiratory Diseases in Children GuideДокумент86 страницRespiratory Diseases in Children Guidemurugesh1969100% (1)
- Pathogen Research AssignmentДокумент2 страницыPathogen Research AssignmentDeven BaliОценок пока нет
- Tuberculosis and The EyeДокумент16 страницTuberculosis and The EyeSaid Plazola MercadoОценок пока нет
- @MedicalBooksStore 2012 (ERS Monograph) TuberculosisДокумент271 страница@MedicalBooksStore 2012 (ERS Monograph) TuberculosisHeri GunawanОценок пока нет
- Harsh PatientReportДокумент1 страницаHarsh PatientReportHarsh GuptaОценок пока нет
- 2009432Документ32 страницы2009432Luis Alberto Letona QuispeОценок пока нет
- Vaccination in PregnancyДокумент7 страницVaccination in PregnancyNoraОценок пока нет
- EpiДокумент3 страницыEpiNiño PaoloОценок пока нет
- Infections of Female Genital TractДокумент67 страницInfections of Female Genital TractSana AftabОценок пока нет
- PathophysiologyДокумент2 страницыPathophysiologySarahlaine BrazasОценок пока нет
- Dafpus IskДокумент4 страницыDafpus IskmarsyaОценок пока нет
- Guidelines For The Use of Fresh-Frozen Plasma, CryoprecipitateДокумент18 страницGuidelines For The Use of Fresh-Frozen Plasma, CryoprecipitatemelaniefarahdillaОценок пока нет
- Ijmr 5 2 179 183Документ5 страницIjmr 5 2 179 183Abhay KumarОценок пока нет