Вам также может понравиться
- A Comparison of Trained and Untrained Vocalists On The Dysphonia Severity Index PDFДокумент6 страницA Comparison of Trained and Untrained Vocalists On The Dysphonia Severity Index PDFAnaОценок пока нет
- INTEGRATION OF SINGING INTO VOICE THERAPY Final Revisions 8-26-09Документ7 страницINTEGRATION OF SINGING INTO VOICE THERAPY Final Revisions 8-26-09Martin SpencerОценок пока нет
- Speak to Win: A Complete Guide to Making Your Voice More Powerful, Pleasant & EffectiveОт EverandSpeak to Win: A Complete Guide to Making Your Voice More Powerful, Pleasant & EffectiveОценок пока нет
- 56.vocal Warmup Log For Belt Your FaceДокумент5 страниц56.vocal Warmup Log For Belt Your FaceAlinutza AlinaОценок пока нет
- Effects On Vocal Fold Collision and PTP of Resonance Tube Phonation With Tube End in Water PDFДокумент10 страницEffects On Vocal Fold Collision and PTP of Resonance Tube Phonation With Tube End in Water PDFIsis Castro ArriolaОценок пока нет
- Resonance StrategiesДокумент11 страницResonance Strategiesdeyse canvaОценок пока нет
- Dysphonic SpeechДокумент4 страницыDysphonic SpeechSooraj SureshkumarОценок пока нет
- Effects of Vocal Training On The AcousticДокумент15 страницEffects of Vocal Training On The AcousticRama RaynsfordОценок пока нет
- The Nursing ShortageДокумент6 страницThe Nursing Shortageapi-455495817Оценок пока нет
- Changes in Glottal Contact Quotient During Resonance Tube Phonation and Phonation With VibratoДокумент7 страницChanges in Glottal Contact Quotient During Resonance Tube Phonation and Phonation With VibratoagcmedsОценок пока нет
- PLAB 2 VISA Guidelines by Omar AlamДокумент18 страницPLAB 2 VISA Guidelines by Omar Alamrafew19Оценок пока нет
- Republic Act No. 10070Документ3 страницыRepublic Act No. 10070Ganiela MCОценок пока нет
- Fundamental Unit of Life 1-25Документ25 страницFundamental Unit of Life 1-25Anisha PanditОценок пока нет
- Tracto Vocal Semiocluido Sus PosturasДокумент4 страницыTracto Vocal Semiocluido Sus PosturasMyriam TokerОценок пока нет
- Source and Filter Adjustments Affecting The Perception of The Vocal Qualities Twang and YawnДокумент10 страницSource and Filter Adjustments Affecting The Perception of The Vocal Qualities Twang and YawnCarol Barrera SaavedraОценок пока нет
- Acoustic Study of Throaty Voice QualityДокумент14 страницAcoustic Study of Throaty Voice QualityVideos Costa Azul100% (1)
- Acoustical and Perceptual Characteristics of Alaryngeal SpeechДокумент59 страницAcoustical and Perceptual Characteristics of Alaryngeal SpeechKUNNAMPALLIL GEJO JOHN100% (1)
- Semi Occluded Vocal Tract Exercises AeroДокумент11 страницSemi Occluded Vocal Tract Exercises AeroSerginho KabuloОценок пока нет
- Chapter 6-Phonation II - PrintVersionДокумент8 страницChapter 6-Phonation II - PrintVersionampiccaОценок пока нет
- Vocal Pitch-Intensity Relationships in Cleft Palate SpeakersДокумент12 страницVocal Pitch-Intensity Relationships in Cleft Palate SpeakersamyyyОценок пока нет
- 7 Tecn Del TVSOДокумент7 страниц7 Tecn Del TVSOKaren Arce RosselОценок пока нет
- Ajustes Del Habla para La Acústica de La Sala y Sus Efectos en El Esfuerzo VocalДокумент26 страницAjustes Del Habla para La Acústica de La Sala y Sus Efectos en El Esfuerzo VocalSALSA 10Оценок пока нет
- Rosemary Lester-Smith - Lester-Smith - Effects of Voice Adjustments On Vocal Tremor and VibratoДокумент15 страницRosemary Lester-Smith - Lester-Smith - Effects of Voice Adjustments On Vocal Tremor and VibratoLore ZazpiОценок пока нет
- Nwav41 NasalДокумент41 страницаNwav41 NasalIgor ReinaОценок пока нет
- Third Class: Neuroscience of Hearing and Speech: NeurolinguisticsДокумент66 страницThird Class: Neuroscience of Hearing and Speech: NeurolinguisticsAniaОценок пока нет
- Fine Structure of Hearing Threshold andДокумент15 страницFine Structure of Hearing Threshold andJuan Sebas Vizuete100% (1)
- 1259 Gilman Marina PDFДокумент2 страницы1259 Gilman Marina PDFIván Zamorano RevecoОценок пока нет
- University of Education LahoreДокумент31 страницаUniversity of Education LahoreSania AshirОценок пока нет
- MDVPДокумент10 страницMDVPCarlos Carrasco Venegas100% (1)
- Lecture 1-7: Source-Filter ModelДокумент6 страницLecture 1-7: Source-Filter ModelhadaspeeryОценок пока нет
- Posturas Semiocluidas Tracto VocalДокумент15 страницPosturas Semiocluidas Tracto VocalKMAОценок пока нет
- Ingo Vocal LoudnessДокумент6 страницIngo Vocal Loudnessmariola_joplinОценок пока нет
- Debit 07Документ8 страницDebit 07Clem LfОценок пока нет
- Kaneko (2015) Multidimensional Analysis On The Effect of VFE On Aged Vocal Fold AtrophyДокумент7 страницKaneko (2015) Multidimensional Analysis On The Effect of VFE On Aged Vocal Fold AtrophyRoberto Martinez SandovalОценок пока нет
- Comparison of Habitual and High Pitch Phonation in Teachers With and Without Vocal FatigueДокумент9 страницComparison of Habitual and High Pitch Phonation in Teachers With and Without Vocal FatiguerosnahsarahsaitОценок пока нет
- Harvard Linguistics 115a Lecture SlidesДокумент29 страницHarvard Linguistics 115a Lecture SlidesJОценок пока нет
- V PhysiologyДокумент0 страницV PhysiologyWaqar Ahmed AwanОценок пока нет
- Doi 10.1016 J.jvoice.2005.12.006Документ6 страницDoi 10.1016 J.jvoice.2005.12.006daniel morenoОценок пока нет
- VowelsДокумент43 страницыVowelskeihoina keihoinaОценок пока нет
- Research Inventy: International Journal of Engineering and ScienceДокумент6 страницResearch Inventy: International Journal of Engineering and ScienceinventyОценок пока нет
- Human Mods 2Документ51 страницаHuman Mods 2Ivan AvramovОценок пока нет
- Three-Dimensional Vocal Tract Imaging and Formant Structure: Varying Vocal Register, Pitch, and LoudnessДокумент6 страницThree-Dimensional Vocal Tract Imaging and Formant Structure: Varying Vocal Register, Pitch, and LoudnessVusala HasanovaОценок пока нет
- 2007, Simberg, The Resonance Tube, Logo Phoniat VocologyДокумент7 страниц2007, Simberg, The Resonance Tube, Logo Phoniat VocologyCarol PaesОценок пока нет
- Phonological Performance in Gerontological SpeechДокумент9 страницPhonological Performance in Gerontological SpeechpaulyfonoОценок пока нет
- High-Frequency Distortion-Product Otoacoustic Emission Repeatability in A Patient PopulationДокумент16 страницHigh-Frequency Distortion-Product Otoacoustic Emission Repeatability in A Patient PopulationCamila Santis MuñozОценок пока нет
- The Singer's Formant and Speaker's Ring Resonance: A Long-Term Average Spectrum AnalysisДокумент5 страницThe Singer's Formant and Speaker's Ring Resonance: A Long-Term Average Spectrum Analysisarts.lamiaaaldawyОценок пока нет
- PsychoPhisics, ExperimentsДокумент9 страницPsychoPhisics, ExperimentsMaria Isabel BinimelisОценок пока нет
- Impact 48 13adoДокумент43 страницыImpact 48 13adoDerib AdoОценок пока нет
- Computerized Tomography Measures DuringДокумент10 страницComputerized Tomography Measures DuringRachelОценок пока нет
- 28 Somashekara EtalДокумент6 страниц28 Somashekara EtaleditorijmrhsОценок пока нет
- EEE 6211 Digital Speech Processing: Course Instructor Dr. Mohammad Ariful Haque Professor, Dept. of EEE, BUETДокумент38 страницEEE 6211 Digital Speech Processing: Course Instructor Dr. Mohammad Ariful Haque Professor, Dept. of EEE, BUETShoaib SamiОценок пока нет
- Intonation For FluencyДокумент50 страницIntonation For Fluencykeihoina keihoinaОценок пока нет
- Peters 1998Документ11 страницPeters 1998Liem NguyenОценок пока нет
- Dissertation Handout.5.7.21Документ12 страницDissertation Handout.5.7.21Kathleen BellОценок пока нет
- Analysis of Stop Consonant Production in EuropeanДокумент5 страницAnalysis of Stop Consonant Production in Europeanxinh nguyenОценок пока нет
- Posturas Semiocluidas Tracto VocalДокумент10 страницPosturas Semiocluidas Tracto VocalKMAОценок пока нет
- Soedersten 2005 Loud Speech in Realistic Environmental Noise - Phonetogram Data, Perceptual Voice Quality, Subjective Ratings, and Gender Differences in Healthy SpeakersДокумент18 страницSoedersten 2005 Loud Speech in Realistic Environmental Noise - Phonetogram Data, Perceptual Voice Quality, Subjective Ratings, and Gender Differences in Healthy SpeakersAna BrankovićОценок пока нет
- Lecture 3 Articulatory PhoneticsДокумент29 страницLecture 3 Articulatory Phoneticsdavegreenwood100% (1)
- Speech Assessment and Nasopharyngoscopy HO 11 07 11Документ164 страницыSpeech Assessment and Nasopharyngoscopy HO 11 07 11catatutuОценок пока нет
- Long-Term Average Spectrum in Screening of Voice Quality in Speech: Untrained Male University StudentsДокумент6 страницLong-Term Average Spectrum in Screening of Voice Quality in Speech: Untrained Male University StudentsMaría Belén Soto AlarcónОценок пока нет
- 1.0 Introduction To Speech ProcessingДокумент40 страниц1.0 Introduction To Speech ProcessingVenkatesh KumarОценок пока нет
- Alta Frecuencia Normativa InternacionalДокумент16 страницAlta Frecuencia Normativa InternacionalAndres DurangoОценок пока нет
- Speaking in Noise - How Does The Lombard Effect Improve Acoustic Contrasts Between Speech and Ambient NoiseДокумент18 страницSpeaking in Noise - How Does The Lombard Effect Improve Acoustic Contrasts Between Speech and Ambient NoiseAna BrankovićОценок пока нет
- Cepstrum y NodulosДокумент3 страницыCepstrum y NodulosSebastian Castro TigheОценок пока нет
- ARTIGO - Efeitos Do Gargarejo - Effects of Voiced Gargling On The Electrical Activity of Extrinsic Laryngeal Muscles and Vocal Self-AssessmentДокумент8 страницARTIGO - Efeitos Do Gargarejo - Effects of Voiced Gargling On The Electrical Activity of Extrinsic Laryngeal Muscles and Vocal Self-AssessmentCarol BarbozaОценок пока нет
- Narrative Pathophysiology of PregnancyДокумент2 страницыNarrative Pathophysiology of PregnancyMarvin ChulyaoОценок пока нет
- Water Security STD 9th Textbook by Techy BagДокумент86 страницWater Security STD 9th Textbook by Techy Bagpooja TiwariОценок пока нет
- Upper Gi f1 Survival GuideДокумент1 страницаUpper Gi f1 Survival GuideNathan Hovis JeffreysОценок пока нет
- AudiometerДокумент3 страницыAudiometerVasanth VasanthОценок пока нет
- PROJECT PROPOSAL AND PROJECT MANAGEMENT TOOLS GROUPWORK (Situation No. 3 - BSSW 3A)Документ21 страницаPROJECT PROPOSAL AND PROJECT MANAGEMENT TOOLS GROUPWORK (Situation No. 3 - BSSW 3A)Hermida Julia AlexandreaОценок пока нет
- Io (Jupiter Moon)Документ2 страницыIo (Jupiter Moon)FatimaОценок пока нет
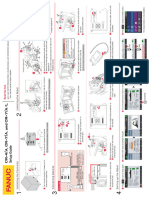
- CR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)Документ1 страницаCR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)lidiia.pavlkukОценок пока нет
- Excerpts From Roe v. Wade Majority OpinionДокумент2 страницыExcerpts From Roe v. Wade Majority OpinioncatherinewangcОценок пока нет
- Neurovascular Assessment PDFДокумент5 страницNeurovascular Assessment PDFNasrullah UllahОценок пока нет
- Diagnostic Test 12Документ3 страницыDiagnostic Test 12Honorato BugayongОценок пока нет
- Hedayati2014 Article BirdStrikeAnalysisOnATypicalHeДокумент12 страницHedayati2014 Article BirdStrikeAnalysisOnATypicalHeSharan KharthikОценок пока нет
- Datasheet Cofraplus 60Документ2 страницыDatasheet Cofraplus 60Žarko JanjićОценок пока нет
- CA500Документ3 страницыCA500Muhammad HussainОценок пока нет
- Emissivity Table E4Документ11 страницEmissivity Table E4Mekro Permana PinemОценок пока нет
- Annual Sustainability Report 2022-23 FinalДокумент93 страницыAnnual Sustainability Report 2022-23 FinalLakshay JajuОценок пока нет
- Industrial SpecialtiesДокумент103 страницыIndustrial SpecialtiesRahul ThekkiniakathОценок пока нет
- QUIZ7 Audit of LiabilitiesДокумент3 страницыQUIZ7 Audit of LiabilitiesCarmela GulapaОценок пока нет
- Figs Taste Scale of Selected Varieties From Hawaiifruit-Net PDFДокумент4 страницыFigs Taste Scale of Selected Varieties From Hawaiifruit-Net PDFHanafizar Hanafi Napi AtanОценок пока нет
- 03 - Air Ticket Request & Claim Form 2018Документ1 страница03 - Air Ticket Request & Claim Form 2018Danny SolvanОценок пока нет
- Dryden, 1994Документ17 страницDryden, 1994Merve KurunОценок пока нет
- Congenital Malformation of The Lung and AirwaysДокумент48 страницCongenital Malformation of The Lung and AirwaysrubyniОценок пока нет
- ProjectxДокумент8 страницProjectxAvinash KumarОценок пока нет
- WWW - Devicemanuals.eu: GardenaДокумент6 страницWWW - Devicemanuals.eu: GardenapotoculОценок пока нет
- Lecture 2 Types of Fluid FlowДокумент29 страницLecture 2 Types of Fluid FlowMilkias endashawОценок пока нет
- Timberwolf TW 230DHB Wood Chipper Instruction ManualДокумент59 страницTimberwolf TW 230DHB Wood Chipper Instruction Manualthuan100% (1)