Вам также может понравиться
- Presented By: Medicine Unit 1Документ95 страницPresented By: Medicine Unit 1Abdullah Muceddidi100% (1)
- 97Документ79 страниц97HATLERОценок пока нет
- Assembling Your Antenna SystemДокумент27 страницAssembling Your Antenna SystemKam MusОценок пока нет
- Ascites: Pathogenesis and Clinical ApproachДокумент34 страницыAscites: Pathogenesis and Clinical ApproachPooja ShashidharanОценок пока нет
- PancreatitisДокумент59 страницPancreatitisAarif RanaОценок пока нет
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesОт EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesОценок пока нет
- AscitesДокумент36 страницAscitesmiki0% (1)
- Soil ResistivityДокумент6 страницSoil ResistivityAnonymous EP0GKhfОценок пока нет
- Hepatobiliary DiseaseДокумент60 страницHepatobiliary DiseaseFirdaus AslamОценок пока нет
- Pressuremeter TestДокумент33 страницыPressuremeter TestHo100% (1)
- Ms Reviewer Renal UrinaryДокумент5 страницMs Reviewer Renal UrinaryAlyssa Nicole CajayonОценок пока нет
- Upper Gi BleedingДокумент37 страницUpper Gi Bleedingfathima AlfasОценок пока нет
- Chapter 3 Rotation and Revolution NotesДокумент12 страницChapter 3 Rotation and Revolution NotesMERLIN ANTHONYОценок пока нет
- With Ordinary Talent and Extraordinary Perseverance, All Things Are Attainable.Документ72 страницыWith Ordinary Talent and Extraordinary Perseverance, All Things Are Attainable.Darin MonerОценок пока нет
- Examination of AbdomenДокумент41 страницаExamination of AbdomenMohammad_Islam87Оценок пока нет
- Approach To Cholestatic Jaundice: DR - Ram Raut - JR III (Medicine) Guide - Dr.D.B. Kadam Seminar Teacher-Dr - NitinДокумент68 страницApproach To Cholestatic Jaundice: DR - Ram Raut - JR III (Medicine) Guide - Dr.D.B. Kadam Seminar Teacher-Dr - NitinAnan JaiswalОценок пока нет
- Cirrhosis of LiverДокумент106 страницCirrhosis of LiveraahadОценок пока нет
- 2015.15009.fundamental Principles of Physical Chemistry - Text PDFДокумент782 страницы2015.15009.fundamental Principles of Physical Chemistry - Text PDFAnoif Naputo Aidnam100% (1)
- Abdominal Sweliing and AscitesДокумент72 страницыAbdominal Sweliing and AscitesFernando Aniban100% (1)
- DLL English 7-10, Week 1 Q1Документ8 страницDLL English 7-10, Week 1 Q1Nemfa TumacderОценок пока нет
- Lecture 20 CarcinogenesisДокумент84 страницыLecture 20 CarcinogenesisMohammad_Islam87100% (1)
- Liver CirrohosisДокумент157 страницLiver CirrohosisSeema SachdevaОценок пока нет
- Liver Cirrhosis: By: Bandna Kumari M.SC (N) 1 YRДокумент66 страницLiver Cirrhosis: By: Bandna Kumari M.SC (N) 1 YRrSОценок пока нет
- Stomach - GastritisДокумент22 страницыStomach - GastritisaimanОценок пока нет
- Liver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisДокумент35 страницLiver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisMohd Johari Mohd ShafuwanОценок пока нет
- Ascites New and ManagementДокумент29 страницAscites New and ManagementANENA RHODAОценок пока нет
- Tutorial Liver FailureДокумент59 страницTutorial Liver FailureNadhrah zulkifliОценок пока нет
- Cirrhosis: LT Col Ravi KanthДокумент33 страницыCirrhosis: LT Col Ravi Kanthravi rajОценок пока нет
- Cirrhosis 22008 Bajar Musica Gratis Descargar Musica Gratis Online Descargar Musica Gratis para CelularesДокумент72 страницыCirrhosis 22008 Bajar Musica Gratis Descargar Musica Gratis Online Descargar Musica Gratis para CelularesYeni Chie Aneuk TuleutОценок пока нет
- With Ordinary Talent and Extraordinary Perseverance, All Things Are Attainable.Документ72 страницыWith Ordinary Talent and Extraordinary Perseverance, All Things Are Attainable.Ainun JaariahОценок пока нет
- NCM Lecture (Liver and Gallbladder)Документ76 страницNCM Lecture (Liver and Gallbladder)beer_ettaaОценок пока нет
- Ascietes by DR Naila MasoodДокумент45 страницAscietes by DR Naila MasoodmichelleОценок пока нет
- Cirrhosis AndrewДокумент33 страницыCirrhosis Andrewlionel andreaОценок пока нет
- CirrhosisДокумент55 страницCirrhosisFUTURE DOCTORОценок пока нет
- DCLDДокумент36 страницDCLDAnonymous uoxEU3mkОценок пока нет
- OUM Tutorial 1 SBNS3504 RenalДокумент51 страницаOUM Tutorial 1 SBNS3504 RenalMashanimy HoneyОценок пока нет
- Cirrhosis - Symptoms, Causes, Stages, Diagnosis, and TreatmentДокумент8 страницCirrhosis - Symptoms, Causes, Stages, Diagnosis, and TreatmentJubitta JobyОценок пока нет
- 3 Liver CirrhosisДокумент50 страниц3 Liver CirrhosisKamal AhmedОценок пока нет
- Renal Function TestsДокумент38 страницRenal Function TestsSupriya NayakОценок пока нет
- Pancreatitis & Pseudocyst in ChildrenДокумент56 страницPancreatitis & Pseudocyst in ChildrendrkiranmОценок пока нет
- Liver CirrhosisДокумент9 страницLiver CirrhosismedsmracelisОценок пока нет
- AscitesДокумент32 страницыAscitesIsaac MwangiОценок пока нет
- Askep SirosisДокумент73 страницыAskep SirosisRisma Yuliana PratiwiОценок пока нет
- Ascites PresentationДокумент19 страницAscites PresentationDanielle FosterОценок пока нет
- What? Who?: DR - Mabel Sihombing Sppd-Kgeh DR - Ilhamd SPPD Dpertemen Ilmu Penyakit Dalam Rs - Ham/Fk-Usu MedanДокумент45 страницWhat? Who?: DR - Mabel Sihombing Sppd-Kgeh DR - Ilhamd SPPD Dpertemen Ilmu Penyakit Dalam Rs - Ham/Fk-Usu MedanM Rizky Assilmy LubisОценок пока нет
- CHOLECYSTITISДокумент6 страницCHOLECYSTITISAnar ChuluunОценок пока нет
- SHS.420 Lec-10: Dr. M.NaumanДокумент39 страницSHS.420 Lec-10: Dr. M.NaumanRehan AbdullahОценок пока нет
- Abd Distension & Ascites-1, All NewДокумент34 страницыAbd Distension & Ascites-1, All NewANENA RHODAОценок пока нет
- Abd Distension & Ascites-2, All You NeedДокумент36 страницAbd Distension & Ascites-2, All You NeedANENA RHODAОценок пока нет
- Renal EmergenciesДокумент93 страницыRenal EmergenciesShubham gaurОценок пока нет
- Laboratory Interpretation Made Easy: Diana Tamondong-Lachica, MD, FPCPДокумент41 страницаLaboratory Interpretation Made Easy: Diana Tamondong-Lachica, MD, FPCPmarieОценок пока нет
- Sirosis Hepatis: Sigit Widyatmoko Fakultas Kedokteran UMSДокумент66 страницSirosis Hepatis: Sigit Widyatmoko Fakultas Kedokteran UMSArif Rahman DmОценок пока нет
- L25 CLD-2Документ55 страницL25 CLD-2S sОценок пока нет
- Acute Renal FailureДокумент20 страницAcute Renal FailureRufus RajОценок пока нет
- Medicine 1Документ114 страницMedicine 1Prajwal P ShetОценок пока нет
- GIT Cirrhosis Liver in ChildrenДокумент37 страницGIT Cirrhosis Liver in ChildrenDr.P.NatarajanОценок пока нет
- Cirrhosis and Its Complications Part 1 LenchoДокумент76 страницCirrhosis and Its Complications Part 1 Lenchoosman nurОценок пока нет
- Liver, Biliary Tract and Pancreas ProblemsДокумент95 страницLiver, Biliary Tract and Pancreas ProblemsBav VAansoqnuaetzОценок пока нет
- Neonatal Cholestasis 2Документ28 страницNeonatal Cholestasis 2HafsaJabbarОценок пока нет
- Jaundice MasterДокумент76 страницJaundice MasterSuresh Kubavat100% (3)
- Renal Faliure 1Документ50 страницRenal Faliure 1180045Оценок пока нет
- Hepatic Disorders: R2 Thanaporn ChittipanichДокумент42 страницыHepatic Disorders: R2 Thanaporn ChittipanichMimmey Yeniw100% (1)
- Cirrhosis Hepatic: DinadewisliДокумент47 страницCirrhosis Hepatic: DinadewisliwilmaОценок пока нет
- 6 Kuliah Liver CirrhosisДокумент55 страниц6 Kuliah Liver CirrhosisAnonymous vUEDx8100% (1)
- The Hepatorenal Syndrome: 11 Pathophysiology and Treatment Ofascites andДокумент27 страницThe Hepatorenal Syndrome: 11 Pathophysiology and Treatment Ofascites andJose JulcaОценок пока нет
- Lecture On Conjugated HyperbilirubinaemiaДокумент38 страницLecture On Conjugated HyperbilirubinaemiaIgwe SolomonОценок пока нет
- AscitesДокумент71 страницаAscitessohilaw210Оценок пока нет
- Bile, Bile Duct and Pancreatic DiseaseДокумент82 страницыBile, Bile Duct and Pancreatic Diseaseshahrul rahmanОценок пока нет
- AnaemiaДокумент83 страницыAnaemiaMohammad_Islam87100% (2)
- Morphopathology SET 16 Pathologies of The Gastrointestinal TractДокумент29 страницMorphopathology SET 16 Pathologies of The Gastrointestinal TractMohammad_Islam87Оценок пока нет
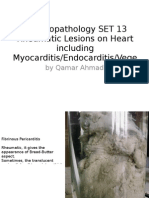
- Morphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeДокумент25 страницMorphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeMohammad_Islam87Оценок пока нет
- Morphopathology SET 15 Renal Pathologies: by Qamar AhmadДокумент25 страницMorphopathology SET 15 Renal Pathologies: by Qamar AhmadMohammad_Islam87Оценок пока нет
- Morphopathology Macroscopy (Romanian-Batch)Документ187 страницMorphopathology Macroscopy (Romanian-Batch)Mohammad_Islam87100% (1)
- Morphopathology SET14 Respiratory Pathologies: by Qamar AhmadДокумент18 страницMorphopathology SET14 Respiratory Pathologies: by Qamar AhmadMohammad_Islam87Оценок пока нет
- ?#ry%oefr: - J4 @,8/ MryДокумент15 страниц?#ry%oefr: - J4 @,8/ MryMohammad_Islam87Оценок пока нет
- Borcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarДокумент7 страницBorcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87100% (1)
- Morphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadДокумент19 страницMorphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadMohammad_Islam87Оценок пока нет
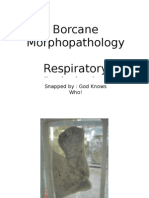
- Borcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarДокумент11 страницBorcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Оценок пока нет
- Borcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarДокумент7 страницBorcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Оценок пока нет
- Workshop 17Документ4 страницыWorkshop 17Mohammad_Islam87Оценок пока нет
- Morphopatholgy Set 9 Circulatory Disturbances: by Qamar AhmadДокумент24 страницыMorphopatholgy Set 9 Circulatory Disturbances: by Qamar AhmadMohammad_Islam87Оценок пока нет
- Workshop 19Документ3 страницыWorkshop 19Mohammad_Islam87Оценок пока нет
- Workshop 20Документ2 страницыWorkshop 20Mohammad_Islam87Оценок пока нет
- Conditions Presenting With Abdominal PainДокумент69 страницConditions Presenting With Abdominal PainaimanОценок пока нет
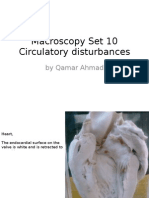
- Macroscopy Set 10 Circulatory Disturbances: by Qamar AhmadДокумент55 страницMacroscopy Set 10 Circulatory Disturbances: by Qamar AhmadMohammad_Islam87Оценок пока нет
- Physical Signs of The AbdomenДокумент93 страницыPhysical Signs of The AbdomenaimanОценок пока нет
- Morphopathology Set 8 Melanocytic Tumors: by Qamar AhmadДокумент54 страницыMorphopathology Set 8 Melanocytic Tumors: by Qamar AhmadMohammad_Islam87Оценок пока нет
- Morphopathology Set 11 Atherosclerosis and Other Cardiaovascular DisordersДокумент21 страницаMorphopathology Set 11 Atherosclerosis and Other Cardiaovascular DisordersMohammad_Islam87Оценок пока нет
- Workshop 18Документ4 страницыWorkshop 18Mohammad_Islam87Оценок пока нет
- STOMACCURS2Документ12 страницSTOMACCURS2Mohammad_Islam87Оценок пока нет
- Peptic Ulcer DiseaseДокумент54 страницыPeptic Ulcer DiseaseMohammad_Islam87Оценок пока нет
- Ben ChanДокумент2 страницыBen ChanAlibabaОценок пока нет
- 4612 4621 Vitamin D Supplementation For Osteoporosis in Older AdultsДокумент10 страниц4612 4621 Vitamin D Supplementation For Osteoporosis in Older AdultsMohammedОценок пока нет
- 12 - Community OutreachДокумент3 страницы12 - Community OutreachAdam ThimmigОценок пока нет
- Check To Make Sure You Have The Most Recent Set of AWS Simple Icons Creating DiagramsДокумент48 страницCheck To Make Sure You Have The Most Recent Set of AWS Simple Icons Creating DiagramsarunchockanОценок пока нет
- 2-Amino-5-Aryl-2-Oxazolines.: (,ee TableДокумент7 страниц2-Amino-5-Aryl-2-Oxazolines.: (,ee TableChristopher HowellОценок пока нет
- Contemporary Philippine MusicДокумент11 страницContemporary Philippine MusicmattyuuОценок пока нет
- BasicsДокумент1 страницаBasicsRishi Raj100% (1)
- Akebono NVH White PaperДокумент4 страницыAkebono NVH White Paperapi-3702571100% (1)
- User Guide: Echolife Hg520C Home GatewayДокумент25 страницUser Guide: Echolife Hg520C Home Gatewayluis PavilaОценок пока нет
- RK3066 Mid PDFДокумент17 страницRK3066 Mid PDFSharon MurphyОценок пока нет
- Shib Mandir, PO-Kadamtala Dist-Darjeeling WB - 734011 JC 18, 3RD Floor, Sector - III Salt Lake City, Kolkata 700098Документ7 страницShib Mandir, PO-Kadamtala Dist-Darjeeling WB - 734011 JC 18, 3RD Floor, Sector - III Salt Lake City, Kolkata 700098Rohit DhanukaОценок пока нет
- Kbli 2017 - 1Документ50 страницKbli 2017 - 1Putri NadiaОценок пока нет
- Shock Cat 2009Документ191 страницаShock Cat 2009gersonplovasОценок пока нет
- RCU II Open Protocol Communication Manual FV 9 10 31 08 PDFДокумент17 страницRCU II Open Protocol Communication Manual FV 9 10 31 08 PDFAndrés ColmenaresОценок пока нет
- FeCl3 Msds - VISCOSITYДокумент9 страницFeCl3 Msds - VISCOSITYramkesh rathaurОценок пока нет
- Hamilton-Resume 4Документ1 страницаHamilton-Resume 4api-654686470Оценок пока нет
- What Is NanoWatt TechnologyДокумент1 страницаWhat Is NanoWatt Technologyfolk_sharathОценок пока нет
- Table of SpecificationДокумент2 страницыTable of SpecificationAya AlisasisОценок пока нет
- Design Report of STOL Transport AircraftДокумент64 страницыDesign Report of STOL Transport Aircrafthassan wastiОценок пока нет
- 3.6.4 Details of Courses For Nuclear Medicine TechnologyДокумент2 страницы3.6.4 Details of Courses For Nuclear Medicine TechnologyhemendrasingОценок пока нет
- Swot Ananlysis of Fintech CompaniesДокумент7 страницSwot Ananlysis of Fintech CompaniesUyen Le VuОценок пока нет
- Visco GraphДокумент4 страницыVisco GraphwamlinaОценок пока нет
- State Magazine, May 2001Документ38 страницState Magazine, May 2001State MagazineОценок пока нет
- BE 503 - Week 1 - Analysis 7.18.11Документ6 страницBE 503 - Week 1 - Analysis 7.18.11dwoodburyОценок пока нет