Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- 1 - Patogenesis HemorroidДокумент16 страниц1 - Patogenesis HemorroidYuli Setio Budi Prabowo100% (1)
- Nausicaä of The Valley of The WindДокумент2 страницыNausicaä of The Valley of The WindYuli Setio Budi PrabowoОценок пока нет
- Varicoseveinsvishnu 120323090133 Phpapp01Документ61 страницаVaricoseveinsvishnu 120323090133 Phpapp01Yuli Setio Budi PrabowoОценок пока нет
- Veins2 120123093329 Phpapp02Документ49 страницVeins2 120123093329 Phpapp02Yuli Setio Budi PrabowoОценок пока нет
- Malformasi AnorektalДокумент1 страницаMalformasi AnorektalYuli Setio Budi PrabowoОценок пока нет
- Thyroid: Cytopathology and Its Histopathological BasesДокумент49 страницThyroid: Cytopathology and Its Histopathological BasesYuli Setio Budi PrabowoОценок пока нет
- MADRSДокумент3 страницыMADRSYuli Setio Budi PrabowoОценок пока нет
- When You Have Asthma: and If You Have Attacks, There's A Good Chance That They Will Be LessДокумент18 страницWhen You Have Asthma: and If You Have Attacks, There's A Good Chance That They Will Be LessYuli Setio Budi PrabowoОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Cert Firefighterrehab PPT July 2012Документ63 страницыCert Firefighterrehab PPT July 2012Sri NivasОценок пока нет
- Old School Fat LossДокумент2 страницыOld School Fat Lossbouc894Оценок пока нет
- Newborn Screening Continuity Clinic Initial Consult Form Ncr/MimaropaДокумент3 страницыNewborn Screening Continuity Clinic Initial Consult Form Ncr/Mimaropajacqueline licupОценок пока нет
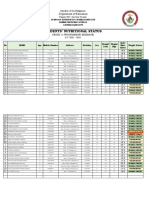
- Students Nutritional Status Template 1Документ4 страницыStudents Nutritional Status Template 1Jeffreynald Arante FranciscoОценок пока нет
- Tacfit 4 DietДокумент13 страницTacfit 4 Dietsaz08100% (2)
- Total Gym WorkoutДокумент8 страницTotal Gym WorkoutOmar Dahan75% (4)
- The Official British Army Fitness Programme: Your 16-Week Planner To Military FitnessДокумент10 страницThe Official British Army Fitness Programme: Your 16-Week Planner To Military FitnessoldskooldaveОценок пока нет
- Applied Strongman Training Part 2Документ48 страницApplied Strongman Training Part 2shaft181100% (2)
- Hormon Reproduksi: Dr. Septi Handayani, M.SiДокумент133 страницыHormon Reproduksi: Dr. Septi Handayani, M.SipiniОценок пока нет
- Macro Recipe Book Vol 3Документ48 страницMacro Recipe Book Vol 3katia100% (1)
- Pathophysiology DKAДокумент2 страницыPathophysiology DKALovely CacapitОценок пока нет
- ICT Project: "Deterrent Malnutrition Among Filipino Children"Документ7 страницICT Project: "Deterrent Malnutrition Among Filipino Children"Janea ArinyaОценок пока нет
- United States Patent: (12) (10) Patent N0.: US 6,586,028 B1Документ14 страницUnited States Patent: (12) (10) Patent N0.: US 6,586,028 B1Anonymous yCfaanqbpQОценок пока нет
- Pre-Test (1 Quarter) Post-Test (4 Quarter) Pre-Test (1 Quarter) Post-Test (4 Quarter)Документ1 страницаPre-Test (1 Quarter) Post-Test (4 Quarter) Pre-Test (1 Quarter) Post-Test (4 Quarter)marynelb270% (1)
- Ejer HipotesisДокумент17 страницEjer HipotesissoryОценок пока нет
- CC3 Final ExamДокумент3 страницыCC3 Final ExamJuitchiboy Nunez DumaoОценок пока нет
- Lecture 11 Evaluation of Diagnostic and Screening Tests Validity and Reliability KanchanaraksaДокумент82 страницыLecture 11 Evaluation of Diagnostic and Screening Tests Validity and Reliability Kanchanaraksapaster125Оценок пока нет
- CLA N Lipid in RuminantsДокумент46 страницCLA N Lipid in RuminantsTamii MatulОценок пока нет
- Lesson Plan 2 Food LabelДокумент33 страницыLesson Plan 2 Food LabelDirgantaraAliifUtamaОценок пока нет
- ABG InterpretationДокумент55 страницABG Interpretationkhoja72Оценок пока нет
- Effective Soccer Coaching DrillsДокумент26 страницEffective Soccer Coaching DrillsAsit GanguliОценок пока нет
- Jason Ferruggia - Renegade Strong PDF-Book Truth & Facts PDFДокумент71 страницаJason Ferruggia - Renegade Strong PDF-Book Truth & Facts PDFbadelog5297100% (1)
- Essay Topic 25Документ35 страницEssay Topic 25گلوبل کنسلٹنٹسОценок пока нет
- Type 2 Diabetes in The Young The Evolving EpidemicДокумент15 страницType 2 Diabetes in The Young The Evolving EpidemicrodtobingОценок пока нет
- Hubungan Asupan Vitamin D Dan Kalsium deДокумент8 страницHubungan Asupan Vitamin D Dan Kalsium detami ariyasraОценок пока нет
- Growth and Development of British Vegan Children - Tom Sanders, AmJClinNutr 1988Документ4 страницыGrowth and Development of British Vegan Children - Tom Sanders, AmJClinNutr 1988Richard PatonОценок пока нет
- 4th Floor Ncp-Part 2Документ2 страницы4th Floor Ncp-Part 2Angel San Pedro CalunsagОценок пока нет
- Counseling Case PresentationДокумент17 страницCounseling Case Presentationapi-348037002Оценок пока нет
- Eddy Wirawan, SPJP - Fiha: Rsud. Ulin BanjarmasinДокумент49 страницEddy Wirawan, SPJP - Fiha: Rsud. Ulin Banjarmasineka febriantyОценок пока нет
- 001 1 PassionFruit - PresentationДокумент8 страниц001 1 PassionFruit - PresentationPeru2007Оценок пока нет