Вам также может понравиться
- Hip Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentОт EverandHip Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentОценок пока нет
- Total Knee ReplacementДокумент9 страницTotal Knee ReplacementFaisal QureshiОценок пока нет
- Trochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandTrochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Orthopedic History Taking: DR - Kholoud Al-ZainДокумент30 страницOrthopedic History Taking: DR - Kholoud Al-ZainKaizar EnnisОценок пока нет
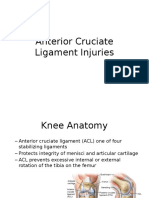
- Anterior Cruciate Ligament InjuriesДокумент16 страницAnterior Cruciate Ligament InjuriesAlmas PrawotoОценок пока нет
- Approach To A Patient With Low Back Ache: DR - Ankur BatraДокумент104 страницыApproach To A Patient With Low Back Ache: DR - Ankur BatraAnkur Batra100% (1)
- Low Back Pain Presentation IMPДокумент114 страницLow Back Pain Presentation IMPrapannika100% (3)
- Orthopath Final ReviewДокумент16 страницOrthopath Final ReviewharrischoeОценок пока нет
- Bio Mechanics and Motor Control of Human Movement 4editionДокумент13 страницBio Mechanics and Motor Control of Human Movement 4editionStanko.Stuhec8307100% (2)
- Prosthetic GaitДокумент33 страницыProsthetic GaitDibyendu DuttaОценок пока нет
- Achilles RuptureДокумент23 страницыAchilles RupturePhysiotherapist AliОценок пока нет
- Examination of The Hip Joint - RP's Ortho NotesДокумент5 страницExamination of The Hip Joint - RP's Ortho NotesSabari NathОценок пока нет
- Clinical Signs - NamedДокумент9 страницClinical Signs - NamedsprapurОценок пока нет
- Distal Biceps Repair Rehabilitation Protocol by Tendayi MutsopotsiДокумент5 страницDistal Biceps Repair Rehabilitation Protocol by Tendayi MutsopotsiPhysiotherapy Care SpecialistsОценок пока нет
- Physical Therapy Management of Thoracic Outlet SyndromeДокумент4 страницыPhysical Therapy Management of Thoracic Outlet SyndromeYashaswi AОценок пока нет
- Gpe - 017.1 - Orthopaedic ExaminationДокумент3 страницыGpe - 017.1 - Orthopaedic ExaminationImiey Eleena HanumОценок пока нет
- Red Flag: MSK Services Pathway - Shoulder PathologyДокумент11 страницRed Flag: MSK Services Pathway - Shoulder PathologyMuhammed ElgasimОценок пока нет
- Orthopaedic Physical ExaminationДокумент94 страницыOrthopaedic Physical ExaminationPriza RazunipОценок пока нет
- Neck PainДокумент1 страницаNeck PainHasan RahmanОценок пока нет
- Perthes Disease: A Rare Childhood Hip ConditionДокумент4 страницыPerthes Disease: A Rare Childhood Hip ConditionMohamed HamoodОценок пока нет
- By Sweta Kumari Summer Project-II Submitted ToДокумент22 страницыBy Sweta Kumari Summer Project-II Submitted ToSudarshanKumar0% (1)
- SPORTS MEDICINE EXAM MCQДокумент22 страницыSPORTS MEDICINE EXAM MCQVolc100% (1)
- Pes Planus and Pes CavusДокумент3 страницыPes Planus and Pes CavusAloysius RodriguesОценок пока нет
- Screening The Sacrum, Sacroiliac, and PelvisДокумент35 страницScreening The Sacrum, Sacroiliac, and PelvisWalijaОценок пока нет
- Classical Disc Herniation by DR Anupreet BassiДокумент17 страницClassical Disc Herniation by DR Anupreet Bassidr_bassiОценок пока нет
- C SpineДокумент33 страницыC SpineKarthickОценок пока нет
- Introduction PhysiotherapistДокумент12 страницIntroduction Physiotherapistapi-371068989Оценок пока нет
- Visual Gait Analysis and Assessment TechniquesДокумент22 страницыVisual Gait Analysis and Assessment TechniquesKumar RanjanОценок пока нет
- Thoracic (Dorsal) SpineДокумент77 страницThoracic (Dorsal) Spineeashoor100% (2)
- Tuberculosis of Hip JointДокумент25 страницTuberculosis of Hip JointYousra ShaikhОценок пока нет
- 2 Hip Examination - How To Examine Hip DR Prof Anil AroraДокумент112 страниц2 Hip Examination - How To Examine Hip DR Prof Anil AroraSaikatОценок пока нет
- Chest cavity, vertebral column and back muscles anatomyДокумент35 страницChest cavity, vertebral column and back muscles anatomyOr100% (2)
- Walking Gait-MUSCLES Involved PDFДокумент2 страницыWalking Gait-MUSCLES Involved PDFlexi_2706Оценок пока нет
- Manual Therapy For Musculoskeletal Pain Syndromes, 1st EditionДокумент16 страницManual Therapy For Musculoskeletal Pain Syndromes, 1st EditionMaansi GuptaОценок пока нет
- Scapula Fracture: DR Jaseem ShamsudeenДокумент32 страницыScapula Fracture: DR Jaseem ShamsudeenJaseemshams ThottiyilОценок пока нет
- Abbreviations in PhysiotherapyДокумент53 страницыAbbreviations in PhysiotherapyPhysiotherapist AliОценок пока нет
- MPFL Repair/Reconstruction Rehab ProtocolДокумент2 страницыMPFL Repair/Reconstruction Rehab ProtocolDruga Danut100% (1)
- Shoulder Impingement SyndromeДокумент29 страницShoulder Impingement SyndromeindunksОценок пока нет
- Orthotic Prescription Factors for KAFOДокумент54 страницыOrthotic Prescription Factors for KAFOFERYANDA UTAMI100% (1)
- PathomechanicsДокумент8 страницPathomechanicsMike B AndersonОценок пока нет
- Knee Injury Seminar GroupДокумент96 страницKnee Injury Seminar GroupAqilah Ab RahmanОценок пока нет
- Heel Pain-Plantar Fasciitis: Revision 2014Документ33 страницыHeel Pain-Plantar Fasciitis: Revision 2014Marianinha AlonsoОценок пока нет
- Oh My Painful FOOT!!!: Plantar FasciitisДокумент20 страницOh My Painful FOOT!!!: Plantar FasciitisAsogaa MeteranОценок пока нет
- MMT 6-1Документ20 страницMMT 6-1Mughal ZadiiОценок пока нет
- Tennis Elbow JOSPT ArticleДокумент11 страницTennis Elbow JOSPT ArticleHasan RahmanОценок пока нет
- Orthopedic AssessmentДокумент4 страницыOrthopedic Assessmentkrissh20Оценок пока нет
- Dance Injuries-Foot and AnkleДокумент7 страницDance Injuries-Foot and Ankleapi-198787605100% (1)
- Orthopedic RSUD Panembahan Senopati BantulДокумент28 страницOrthopedic RSUD Panembahan Senopati Bantulwinda alviraОценок пока нет
- Hip & Knee Extremity Notes: Lower Extremity Evaluation Research & Orthopedic TestsДокумент116 страницHip & Knee Extremity Notes: Lower Extremity Evaluation Research & Orthopedic Testsjoe joeОценок пока нет
- Upper Cross SyndromeДокумент3 страницыUpper Cross Syndromecarrotbutter0% (1)
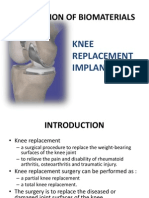
- Application of BiomaterialsДокумент11 страницApplication of BiomaterialsNurmasturaHoney A'Razak100% (1)
- Examination of The Knee Joint - RP's Ortho NotesДокумент3 страницыExamination of The Knee Joint - RP's Ortho NotesSabari NathОценок пока нет
- Clinical Anatomy of Joints of Lower ExtremityДокумент76 страницClinical Anatomy of Joints of Lower ExtremityRabia RafiqueОценок пока нет
- Red Flag: MSK Services Pathway - Hand PathologyДокумент10 страницRed Flag: MSK Services Pathway - Hand PathologyMuhammed ElgasimОценок пока нет
- New Patient Spine PacketДокумент16 страницNew Patient Spine PacketDebra SmithОценок пока нет
- Cervical SpineДокумент177 страницCervical SpineJayaRakMinimarketОценок пока нет
- Hip & Groin Pain DD PDFДокумент15 страницHip & Groin Pain DD PDFagniosaiОценок пока нет
- Assessment of KneeДокумент113 страницAssessment of KneeIqra Iftikhar100% (1)
- Knee Biomechanics: by Amrita..Документ57 страницKnee Biomechanics: by Amrita..Chanda NathaniОценок пока нет
- Money Laundering in Online Trading RegulationДокумент8 страницMoney Laundering in Online Trading RegulationSiti Rabiah MagfirohОценок пока нет
- Statistical Quality Control, 7th Edition by Douglas C. Montgomery. 1Документ76 страницStatistical Quality Control, 7th Edition by Douglas C. Montgomery. 1omerfaruk200141Оценок пока нет
- Guide To Raising Capital From Angel Investors Ebook From The Startup Garage PDFДокумент20 страницGuide To Raising Capital From Angel Investors Ebook From The Startup Garage PDFLars VonTurboОценок пока нет
- Public Private HEM Status AsOn2May2019 4 09pmДокумент24 страницыPublic Private HEM Status AsOn2May2019 4 09pmVaibhav MahobiyaОценок пока нет
- Differential Pulse Code ModulationДокумент12 страницDifferential Pulse Code ModulationNarasimhareddy MmkОценок пока нет
- Damcos Mas2600 Installation UsermanualДокумент26 страницDamcos Mas2600 Installation Usermanualair1111Оценок пока нет
- Role of PAOДокумент29 страницRole of PAOAjay DhokeОценок пока нет
- Critical Methodology Analysis: 360' Degree Feedback: Its Role in Employee DevelopmentДокумент3 страницыCritical Methodology Analysis: 360' Degree Feedback: Its Role in Employee DevelopmentJatin KaushikОценок пока нет
- Test Bank For Fundamental Financial Accounting Concepts 10th by EdmondsДокумент18 страницTest Bank For Fundamental Financial Accounting Concepts 10th by Edmondsooezoapunitory.xkgyo4100% (48)
- CDI-AOS-CX 10.4 Switching Portfolio Launch - Lab V4.01Документ152 страницыCDI-AOS-CX 10.4 Switching Portfolio Launch - Lab V4.01Gilles DellaccioОценок пока нет
- The Service Marketing Plan On " Expert Personalized Chef": Presented byДокумент27 страницThe Service Marketing Plan On " Expert Personalized Chef": Presented byA.S. ShuvoОценок пока нет
- Computer Networks Transmission Media: Dr. Mohammad AdlyДокумент14 страницComputer Networks Transmission Media: Dr. Mohammad AdlyRichthofen Flies Bf109Оценок пока нет
- Meet Joe Black (1998) : A Metaphor of LifeДокумент10 страницMeet Joe Black (1998) : A Metaphor of LifeSara OrsenoОценок пока нет
- Ultra Slimpak G448-0002: Bridge Input Field Configurable IsolatorДокумент4 страницыUltra Slimpak G448-0002: Bridge Input Field Configurable IsolatorVladimirОценок пока нет
- SBI Sample PaperДокумент283 страницыSBI Sample Paperbeintouch1430% (1)
- Srimanta Sankaradeva Universityof Health SciencesДокумент3 страницыSrimanta Sankaradeva Universityof Health SciencesTemple RunОценок пока нет
- Mounting InstructionДокумент1 страницаMounting InstructionAkshay GargОценок пока нет
- Cableado de TermocuplasДокумент3 страницыCableado de TermocuplasRUBEN DARIO BUCHELLYОценок пока нет
- C4 ISRchapterДокумент16 страницC4 ISRchapterSerkan KalaycıОценок пока нет
- Equilibruim of Forces and How Three Forces Meet at A PointДокумент32 страницыEquilibruim of Forces and How Three Forces Meet at A PointSherif Yehia Al MaraghyОценок пока нет
- HP HP3-X11 Exam: A Composite Solution With Just One ClickДокумент17 страницHP HP3-X11 Exam: A Composite Solution With Just One ClicksunnyОценок пока нет
- Composite Structures: A. Grimaldi, A. Sollo, M. Guida, F. MaruloДокумент15 страницComposite Structures: A. Grimaldi, A. Sollo, M. Guida, F. MaruloSharan KharthikОценок пока нет
- Chapter 4 DeterminantsДокумент3 страницыChapter 4 Determinantssraj68Оценок пока нет
- Assembly ModelingДокумент222 страницыAssembly ModelingjdfdfererОценок пока нет
- (123doc) - Chapter-24Документ6 страниц(123doc) - Chapter-24Pháp NguyễnОценок пока нет
- Tutorial 1 Discussion Document - Batch 03Документ4 страницыTutorial 1 Discussion Document - Batch 03Anindya CostaОценок пока нет
- Dolni VestoniceДокумент34 страницыDolni VestoniceOlha PodufalovaОценок пока нет
- THE DOSE, Issue 1 (Tokyo)Документ142 страницыTHE DOSE, Issue 1 (Tokyo)Damage85% (20)
- CALCULUS PHYSICS MIDTERMДокумент41 страницаCALCULUS PHYSICS MIDTERMMACARIO QTОценок пока нет
- SEC QPP Coop TrainingДокумент62 страницыSEC QPP Coop TrainingAbdalelah BagajateОценок пока нет