Вам также может понравиться
- Infective EndocarditisДокумент57 страницInfective EndocarditisRika FitriaОценок пока нет
- EndocarditisДокумент38 страницEndocarditiseviherdiantiОценок пока нет
- Lecture Infective EndocarditisДокумент37 страницLecture Infective EndocarditisJohnson OlawaleОценок пока нет
- Infective EndocarditisДокумент67 страницInfective EndocarditisDr. Rajesh PadhiОценок пока нет
- Infective EndocarditisДокумент45 страницInfective EndocarditisReem 10Оценок пока нет
- Bacterial EndocarditisДокумент14 страницBacterial EndocarditisSubhanAnwarKhanОценок пока нет
- 9 - Invefctive EndocarditiesДокумент71 страница9 - Invefctive EndocarditiesMahmoud OmarОценок пока нет
- 8.29.06 Staphlococcal BacteremiaДокумент41 страница8.29.06 Staphlococcal BacteremiaVaibhav KaroliyaОценок пока нет
- Endocarditis Blok 10Документ50 страницEndocarditis Blok 10Dena Paramita RustandiОценок пока нет
- Modified Duke's Criteria For Infective Endocarditis - Mnemonic - EpomedicineДокумент5 страницModified Duke's Criteria For Infective Endocarditis - Mnemonic - EpomedicineAsmaОценок пока нет
- Infective Endocarditis: History & ExamДокумент75 страницInfective Endocarditis: History & ExamMicija CucuОценок пока нет
- A Case of Acute IdiopathicДокумент19 страницA Case of Acute IdiopathicSAIMA BATOOLОценок пока нет
- Rheumatic Fever: Prof. A K M MohibullahДокумент42 страницыRheumatic Fever: Prof. A K M MohibullahNavojit ChowdhuryОценок пока нет
- Infective Endocarditis: Ainal Fadly Adigama PF Enny SuryantiДокумент50 страницInfective Endocarditis: Ainal Fadly Adigama PF Enny SuryantiFaisal Reza AdiebОценок пока нет
- PEDIA - Acquired Heart DiseaseДокумент5 страницPEDIA - Acquired Heart DiseaseStephen Pilar PortilloОценок пока нет
- Disease of Endocardium, Myocardium and PericardiumДокумент54 страницыDisease of Endocardium, Myocardium and PericardiumadystiОценок пока нет
- Educational Case: Kidney Transplant Rejection: Kevin Kuan, MD and Daniel Schwartz, MDДокумент7 страницEducational Case: Kidney Transplant Rejection: Kevin Kuan, MD and Daniel Schwartz, MDL AОценок пока нет
- Infectious Diseases - Infective EndocarditisДокумент41 страницаInfectious Diseases - Infective Endocarditisfire_n_iceОценок пока нет
- Infective Endocarditis: Uaepong Limpapanasit July 5, 2010Документ45 страницInfective Endocarditis: Uaepong Limpapanasit July 5, 2010Rapid MedicineОценок пока нет
- EndocarditisДокумент53 страницыEndocarditisمحمد ربيعيОценок пока нет
- Febrile Neutropenia Final 7-29Документ74 страницыFebrile Neutropenia Final 7-29Juliyanti FuОценок пока нет
- Fever With A Focus in Well Looking Child Under 3 YrsДокумент80 страницFever With A Focus in Well Looking Child Under 3 YrsAnuradha RoopchandОценок пока нет
- Anak 3.1 Infective Endocarditis DRTLTДокумент21 страницаAnak 3.1 Infective Endocarditis DRTLTAnastasia PinkyОценок пока нет
- Nephritic/nephrotic Syndrome.Документ37 страницNephritic/nephrotic Syndrome.Kelechi OtamiriОценок пока нет
- Amjad Bani Hani: Sir S, Sep S Is, A N D ModsДокумент67 страницAmjad Bani Hani: Sir S, Sep S Is, A N D ModsRuffaeelJabrОценок пока нет
- Bacterial EndocarditisДокумент5 страницBacterial EndocarditisAMOS MELIОценок пока нет
- Infective Endocarditis IeДокумент26 страницInfective Endocarditis IeAnthie FitriОценок пока нет
- SepsisДокумент54 страницыSepsisStayOnSundayОценок пока нет
- Evaluation of The Febrile Patient A Case-Based Approach: Fevers and Fevers of Unknown OriginДокумент97 страницEvaluation of The Febrile Patient A Case-Based Approach: Fevers and Fevers of Unknown Originkrish vjОценок пока нет
- SepsisДокумент54 страницыSepsisStayOnSundayОценок пока нет
- Oncologic Emergencies: Greg V. MansonДокумент43 страницыOncologic Emergencies: Greg V. Mansonalarajpoetry100% (2)
- Lecture 19 - Infective Is Pericarditis and MyocarditisДокумент4 страницыLecture 19 - Infective Is Pericarditis and MyocarditisJane HoОценок пока нет
- IM Infective Endocarditis Pericardial DiseaseДокумент4 страницыIM Infective Endocarditis Pericardial DiseaseLucyellowOttemoesoeОценок пока нет
- Infective Endocarditis: DR - Sri Hastuti SPJP Fiha. Rsud - Dr. M.Yunus BemgkuluДокумент27 страницInfective Endocarditis: DR - Sri Hastuti SPJP Fiha. Rsud - Dr. M.Yunus Bemgkulujulis muharamОценок пока нет
- Infective Endocarditis - Krishna: Investigations and Management ofДокумент25 страницInfective Endocarditis - Krishna: Investigations and Management ofrajkalyОценок пока нет
- Infective EndocarditisДокумент68 страницInfective EndocarditisDr. Rajesh PadhiОценок пока нет
- Infective Endocarditis.... MshembaДокумент39 страницInfective Endocarditis.... MshembaTimothy Casmiry MshembaОценок пока нет
- CVS II Tutorials Apr 12-17Документ7 страницCVS II Tutorials Apr 12-17rishitОценок пока нет
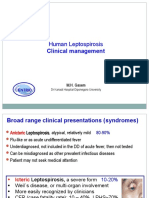
- Lepto Clinical Management GLEAN 2019 - M GasemДокумент42 страницыLepto Clinical Management GLEAN 2019 - M GasemSelfie C RijalОценок пока нет
- ENDOCARDITISДокумент7 страницENDOCARDITIS46 MalsawmtluangiОценок пока нет
- Infective Endocarditis Case ReportДокумент40 страницInfective Endocarditis Case Reportliu_owen17100% (1)
- C29BДокумент1 страницаC29Breny93Оценок пока нет
- Ug Infective Endocarditis SubmitДокумент49 страницUg Infective Endocarditis SubmitAhmed FaizalОценок пока нет
- Sepsis 2013Документ42 страницыSepsis 2013RatnaОценок пока нет
- Is It Always Anterior Chest Pain Angina Pectoris?Документ7 страницIs It Always Anterior Chest Pain Angina Pectoris?Diana MinzatОценок пока нет
- UrosepsisДокумент35 страницUrosepsisdrasas690Оценок пока нет
- 28 EndocarditeleДокумент2 страницы28 Endocarditelecristian241Оценок пока нет
- Duke Criteria For Infective EndocarditisДокумент2 страницыDuke Criteria For Infective EndocarditisandrikeishaОценок пока нет
- General Medicine SEQs SolvedДокумент33 страницыGeneral Medicine SEQs SolvedMajid Ahmed FareaОценок пока нет
- Infective Endocardits: Dr. Abhay Kumar MODERATOR-Dr. Rajesh KumarДокумент42 страницыInfective Endocardits: Dr. Abhay Kumar MODERATOR-Dr. Rajesh KumarAbhay BarnwalОценок пока нет
- 1 Fever of Unknown OriginДокумент33 страницы1 Fever of Unknown Originhamzatrad949Оценок пока нет
- Management of Infective Endocarditis: Valve DiseaseДокумент17 страницManagement of Infective Endocarditis: Valve DiseaseLaura AmaliaОценок пока нет
- Endocarditis ReviewДокумент8 страницEndocarditis ReviewCatherine Saenz SerranoОценок пока нет
- Sbe in ChildrenДокумент42 страницыSbe in Childrengrim reaperОценок пока нет
- New-Infective EndocarditisДокумент30 страницNew-Infective Endocarditisزياد سعيدОценок пока нет
- S Infective EndocarditisДокумент24 страницыS Infective EndocarditisMpanso Ahmad AlhijjОценок пока нет
- Sepsis in PregnancyДокумент25 страницSepsis in Pregnancysana khan008Оценок пока нет
- Microbiology of CVSДокумент44 страницыMicrobiology of CVSsultan khabeebОценок пока нет
- Print Order #145000987Документ1 страницаPrint Order #145000987andreva8Оценок пока нет
- Introduksi Blok Dissaster 21Документ13 страницIntroduksi Blok Dissaster 21andreva8Оценок пока нет
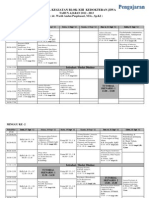
- Jadwal Kegiatan Blok Xiii - 2012-2013Документ4 страницыJadwal Kegiatan Blok Xiii - 2012-2013andreva8Оценок пока нет
- Typhoid Fever: Divisi Tropik Dan Infeksi Bag/Smf - Ilmu Penyakit Dalam FK Unsyiah Rsud. Dr. Zainoel Abidin Banda AcehДокумент23 страницыTyphoid Fever: Divisi Tropik Dan Infeksi Bag/Smf - Ilmu Penyakit Dalam FK Unsyiah Rsud. Dr. Zainoel Abidin Banda Acehandreva8Оценок пока нет
- Cholelithiasis and CholecystitisДокумент28 страницCholelithiasis and Cholecystitisandreva8Оценок пока нет
- sISTEM iMMUNEДокумент62 страницыsISTEM iMMUNEandreva8Оценок пока нет
- Hipertensi: Maimun SyukriДокумент41 страницаHipertensi: Maimun Syukriandreva8Оценок пока нет