Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- 2022 Oxford Handbook of Anaesthesia Oxford Press 5th Edition ExportДокумент2 страницы2022 Oxford Handbook of Anaesthesia Oxford Press 5th Edition ExportHany Elbarougy0% (3)
- Competency Assessment QuestionnaireДокумент2 страницыCompetency Assessment QuestionnairekurutalaОценок пока нет
- BORLAND D. M., Digestive Drugs (Bl6)Документ51 страницаBORLAND D. M., Digestive Drugs (Bl6)ruling_geminiОценок пока нет
- Microbiology A Systems Approach Cowan 4th Edition Test BankДокумент10 страницMicrobiology A Systems Approach Cowan 4th Edition Test BankKathy Gasiewski100% (41)
- Functional Gastrointestinal Disorders History Pathophysiology Clinical Features and Rome IVДокумент20 страницFunctional Gastrointestinal Disorders History Pathophysiology Clinical Features and Rome IVwenyinriantoОценок пока нет
- Ebook John Murtaghs General Practice Companion Handbook PDF Full Chapter PDFДокумент67 страницEbook John Murtaghs General Practice Companion Handbook PDF Full Chapter PDFroberto.duncan209100% (27)
- OET Reading Test 7 - Part BДокумент13 страницOET Reading Test 7 - Part BLOTSOFTESTS80% (5)
- Community Nursing Care PlanДокумент6 страницCommunity Nursing Care Plantansincos93% (14)
- BernottiДокумент44 страницыBernottiAlexandra Alexandra100% (2)
- Regional AnesДокумент36 страницRegional AnesMay Anne BuenafeОценок пока нет
- CBM Impact (April 2014) : Training Manager'S Name: Anil RamakrishnanДокумент2 страницыCBM Impact (April 2014) : Training Manager'S Name: Anil RamakrishnankurutalaОценок пока нет
- Names To Be Deleted From TracerДокумент2 страницыNames To Be Deleted From TracerkurutalaОценок пока нет
- Program Name Division Name Date Duration of Days TimeДокумент2 страницыProgram Name Division Name Date Duration of Days TimekurutalaОценок пока нет
- AnnouncementДокумент1 страницаAnnouncementkurutalaОценок пока нет
- SR No Division Brand: Division Wise Brands For Interview PanelДокумент1 страницаSR No Division Brand: Division Wise Brands For Interview PanelkurutalaОценок пока нет
- DRIVE PROGRAM (2013 - 2014) : Total Total Total TotalДокумент1 страницаDRIVE PROGRAM (2013 - 2014) : Total Total Total TotalkurutalaОценок пока нет
- Healtheon DetailingДокумент1 страницаHealtheon DetailingkurutalaОценок пока нет
- La Shield DetailingДокумент2 страницыLa Shield DetailingkurutalaОценок пока нет
- TOUCH Untrained Status (January 2014)Документ2 страницыTOUCH Untrained Status (January 2014)kurutalaОценок пока нет
- Ascoril Expectorant - Detailing Story InterviewsДокумент2 страницыAscoril Expectorant - Detailing Story InterviewskurutalaОценок пока нет
- Esoz - Detailing TalkДокумент2 страницыEsoz - Detailing TalkkurutalaОценок пока нет
- 08 Drug ProfileДокумент2 страницы08 Drug ProfilekurutalaОценок пока нет
- Yearly Calender CDG ' 12-13 FinalДокумент6 страницYearly Calender CDG ' 12-13 FinalkurutalaОценок пока нет
- Glenmark CV DetailingДокумент1 страницаGlenmark CV DetailingkurutalaОценок пока нет
- CTV DetailingДокумент1 страницаCTV DetailingkurutalaОценок пока нет
- Critica VAF Detailing TalkДокумент1 страницаCritica VAF Detailing TalkkurutalaОценок пока нет
- Activity Report & Monthly Planner - Training Manager - AUGUST'12Документ4 страницыActivity Report & Monthly Planner - Training Manager - AUGUST'12kurutalaОценок пока нет
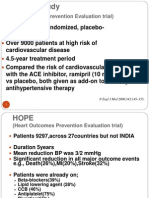
- The HOPE Study: (Heart Outcomes Prevention Evaluation Trial)Документ4 страницыThe HOPE Study: (Heart Outcomes Prevention Evaluation Trial)kurutalaОценок пока нет
- Activity Report & Monthly Planner - Training Manager - April MayДокумент4 страницыActivity Report & Monthly Planner - Training Manager - April MaykurutalaОценок пока нет
- Name of Employee Date of Birth (DD-MM-Yyyy) Contact NumberДокумент3 страницыName of Employee Date of Birth (DD-MM-Yyyy) Contact NumberkurutalaОценок пока нет
- Giant Bowen's Disease On The Face: Case Report and Review of The LiteratureДокумент4 страницыGiant Bowen's Disease On The Face: Case Report and Review of The LiteraturezoeyОценок пока нет
- EMPANELEDHOSPITALLISTДокумент12 страницEMPANELEDHOSPITALLISTVsknОценок пока нет
- Oct Symp AbhiДокумент54 страницыOct Symp AbhiMonisha ArulalanОценок пока нет
- Department of MEDICINE-1Документ16 страницDepartment of MEDICINE-1Ajay BangОценок пока нет
- First Aid Maxilofacl SurgeryДокумент94 страницыFirst Aid Maxilofacl SurgerydoctorniravОценок пока нет
- Clinical Experience With MEBO in Treating Paederus DermatitisДокумент2 страницыClinical Experience With MEBO in Treating Paederus Dermatitissoumalya481Оценок пока нет
- (S-W5-Sun-Gen.S) (By Dr. Emad) Gall Bladder 1Документ28 страниц(S-W5-Sun-Gen.S) (By Dr. Emad) Gall Bladder 1Haider Nadhem AL-rubaiОценок пока нет
- Hypertensive CrisisДокумент13 страницHypertensive Crisis.Katherine CalderonОценок пока нет
- 33rd IACDE National Conference 2018 - VijayawadaДокумент5 страниц33rd IACDE National Conference 2018 - VijayawadaHari PriyaОценок пока нет
- 5 4 3 2 1 Grounding Techniqueqspae PDFДокумент2 страницы5 4 3 2 1 Grounding Techniqueqspae PDFsheetcherry57Оценок пока нет
- Analisis Lama Waktu Pelayanan Laboratorium Di Rumah Sakit Umum Daerah Pasaman BaratДокумент8 страницAnalisis Lama Waktu Pelayanan Laboratorium Di Rumah Sakit Umum Daerah Pasaman Baratdina filanОценок пока нет
- Incise Drapes UK GX750 6pДокумент6 страницIncise Drapes UK GX750 6pbouchra8blsОценок пока нет
- Typhon PAST WorksheetДокумент2 страницыTyphon PAST WorksheetKa Chun NgОценок пока нет
- Tuesday 14 January 2020: BiologyДокумент24 страницыTuesday 14 January 2020: Biologysham80% (5)
- Types of Feeding-GastrostomyДокумент8 страницTypes of Feeding-GastrostomyElda KuizonОценок пока нет
- Pearls ToxocologicДокумент3 страницыPearls ToxocologichsbacongaОценок пока нет
- Vaccination Certificate 20435699572410Документ1 страницаVaccination Certificate 20435699572410MANOJ BHADANEОценок пока нет
- Motor Neurone Disease: J GormallyДокумент14 страницMotor Neurone Disease: J GormallyBambang SutrisnoОценок пока нет
- It Just Makes Sense 2012Документ25 страницIt Just Makes Sense 2012Emf RefugeeОценок пока нет
- Slide Materi Dr. Kevin Triangto, SPKFR - Heart Failure - PMR4GP 2022Документ27 страницSlide Materi Dr. Kevin Triangto, SPKFR - Heart Failure - PMR4GP 2022Maulia Wisda Era ChresiaОценок пока нет
- Opalescence Tooth Whitening Systems: At-Home Whitening InstructionsДокумент1 страницаOpalescence Tooth Whitening Systems: At-Home Whitening InstructionsPande NandaОценок пока нет