Вам также может понравиться
- 81-Article Text-240-1-10-20160110 PDFДокумент26 страниц81-Article Text-240-1-10-20160110 PDFSazzad HossainОценок пока нет
- Supporting Deaf Culture Whilst Looking for a Cure: Conflicting Responses to DeafnessОт EverandSupporting Deaf Culture Whilst Looking for a Cure: Conflicting Responses to DeafnessОценок пока нет
- Syllabus: Need Disability Approaches Development of Universal Design InitiativesДокумент93 страницыSyllabus: Need Disability Approaches Development of Universal Design InitiativesVikasОценок пока нет
- Accessibility of Public Spaces: Case Study of Ikeja, Lagos State, NigeriaДокумент13 страницAccessibility of Public Spaces: Case Study of Ikeja, Lagos State, NigeriainventionjournalsОценок пока нет
- Module - 1 - Barrier FreeДокумент6 страницModule - 1 - Barrier Freefathima noureenОценок пока нет
- CHAPTER 2 Addressing Diversity Through The YearsДокумент4 страницыCHAPTER 2 Addressing Diversity Through The YearsPrincess Kyla SalvadorОценок пока нет
- Synopsis Research Methods 1Документ11 страницSynopsis Research Methods 1Mark TeyeОценок пока нет
- Disability & SocietyДокумент18 страницDisability & Societysdfghalib1Оценок пока нет
- Bridging Ageing and Disability - An IntroductionДокумент8 страницBridging Ageing and Disability - An IntroductionGerald NwekeОценок пока нет
- Barnes Rehab2Документ48 страницBarnes Rehab2Dana Vanina Bustos TorésОценок пока нет
- Study For PCДокумент14 страницStudy For PCDHINESH THIRUMURUGAN (RA1611201010079)Оценок пока нет
- Ellis Goggin 2015 Disability Media Participation Opportunities Obstacles and PoliticsДокумент11 страницEllis Goggin 2015 Disability Media Participation Opportunities Obstacles and PoliticsEduardo GuerraОценок пока нет
- Development Ethics - What? Why ? How?Документ26 страницDevelopment Ethics - What? Why ? How?Roy Salmo Suárez TorrenegraОценок пока нет
- (2013) Des Gasper. Development Ethics. What Why How PDFДокумент26 страниц(2013) Des Gasper. Development Ethics. What Why How PDFCasandra HernandezОценок пока нет
- Achieving an Accessible City for All Through Revision of Urban SpacesДокумент6 страницAchieving an Accessible City for All Through Revision of Urban SpacesSap IensОценок пока нет
- A Working Social Model?: Disability and Work in The 21st CenturyДокумент27 страницA Working Social Model?: Disability and Work in The 21st CenturyJaderson GadonskiОценок пока нет
- Class 1 Introduction To Disability StudiesДокумент16 страницClass 1 Introduction To Disability Studiesaggressive0709Оценок пока нет
- Works On AccessДокумент13 страницWorks On AccessAmudha RathinamОценок пока нет
- Inclusiveness (Chap 3 To 8)Документ40 страницInclusiveness (Chap 3 To 8)dawitshewa4Оценок пока нет
- Wearables and People With Disabilities:: Damara Goff Paris Katrina R. MillerДокумент17 страницWearables and People With Disabilities:: Damara Goff Paris Katrina R. Millernoknok loОценок пока нет
- International Commitments Advance Disability RightsДокумент16 страницInternational Commitments Advance Disability Rightspecot aieОценок пока нет
- IMPETUS Challenge 2 2024 Justice and EquityДокумент3 страницыIMPETUS Challenge 2 2024 Justice and Equitynataliamarin.artaОценок пока нет
- Identifying Social Inclusion and Exclusion: Key MessagesДокумент16 страницIdentifying Social Inclusion and Exclusion: Key MessagesMANINEEОценок пока нет
- The Inclusive City: Delivering A More Accessible Urban Environment Through Inclusive DesignДокумент39 страницThe Inclusive City: Delivering A More Accessible Urban Environment Through Inclusive DesignAyça YalçınОценок пока нет
- DISABILITY AND DEVELOPMENT Robert Metts PDFДокумент45 страницDISABILITY AND DEVELOPMENT Robert Metts PDFNafis Hasan khanОценок пока нет
- Mac ProposalДокумент6 страницMac ProposalelizabetharaujomelaniaОценок пока нет
- Challenging Urban Exclusion? Theory and PracticeДокумент15 страницChallenging Urban Exclusion? Theory and PracticeMichał NowosielskiОценок пока нет
- Geographic Information Systems andДокумент9 страницGeographic Information Systems andRosen AnthonyОценок пока нет
- Disability-Nalars Vol 1 No 2 Juli 2002Документ8 страницDisability-Nalars Vol 1 No 2 Juli 2002Ari WeepeeОценок пока нет
- Lid and Solvang (Dis) Ability and The Experience of Accessibility in The Urban EnvironmentДокумент14 страницLid and Solvang (Dis) Ability and The Experience of Accessibility in The Urban EnvironmentMatt AlteaОценок пока нет
- Inclusiveness ModuleДокумент346 страницInclusiveness ModuleMekuriya BeregaОценок пока нет
- SOCIOДокумент4 страницыSOCIOSharmaineОценок пока нет
- RCI: Access For All - Training Manual Barrier-Free Design, 2005Документ173 страницыRCI: Access For All - Training Manual Barrier-Free Design, 2005Vaishnavi JayakumarОценок пока нет
- Center For Universal DesignДокумент165 страницCenter For Universal DesignMohammed_Safiu_5797Оценок пока нет
- Social Dimension of Urban Design: People, Space, Neighborhoods and SafetyДокумент14 страницSocial Dimension of Urban Design: People, Space, Neighborhoods and SafetyDEXTRO 000Оценок пока нет
- Brynard Challenges (2010)Документ16 страницBrynard Challenges (2010)Gena DuresaОценок пока нет
- Revised Pn-Law Society and Controversy (K9nke4six5) 1Документ12 страницRevised Pn-Law Society and Controversy (K9nke4six5) 1aries usamaОценок пока нет
- 2013 - Message of The International Committee For October 17Документ2 страницы2013 - Message of The International Committee For October 17Donald LeeОценок пока нет
- The Right of Persons With Disabilities To Live in The CommunityДокумент35 страницThe Right of Persons With Disabilities To Live in The CommunityIipo ChennaiОценок пока нет
- Models of Disability and Human Rights: Informing The Improvement of Built Environment Accessibility For People With Disability at Neighborhood Scale?Документ21 страницаModels of Disability and Human Rights: Informing The Improvement of Built Environment Accessibility For People With Disability at Neighborhood Scale?Sai smitaОценок пока нет
- Reviewer MST2 Semi FinalДокумент15 страницReviewer MST2 Semi FinalvctsinvctsОценок пока нет
- Media KitДокумент4 страницыMedia KitReem AlanziОценок пока нет
- Literature Collection For Universal DesignДокумент43 страницыLiterature Collection For Universal DesignRiddhi Sanghvi100% (1)
- Barnes & Mercer 1997Документ13 страницBarnes & Mercer 1997Audrey GarryОценок пока нет
- Disability Rights and Built Environment AccessДокумент25 страницDisability Rights and Built Environment AccessLavana FayeОценок пока нет
- Accessibility in Gaming Literature Review - Brian DuffyДокумент13 страницAccessibility in Gaming Literature Review - Brian DuffyBrian DuffyОценок пока нет
- Changing Social Relations of Disability ResearchДокумент15 страницChanging Social Relations of Disability ResearchDenisson Gonçalves ChavesОценок пока нет
- Universal Design Guide For Inclusive TourismДокумент20 страницUniversal Design Guide For Inclusive TourismScott PruettОценок пока нет
- NSTP ReviewerДокумент13 страницNSTP ReviewerMillicent Belle TolentinoОценок пока нет
- Addis Abeba Science and Technology UniversityДокумент29 страницAddis Abeba Science and Technology Universityberhaneselassie wobeshetОценок пока нет
- All Lectures SociologyДокумент84 страницыAll Lectures SociologyImtiaz uddin MahiОценок пока нет
- LIDO - Activism and The Academy Losing The Ideological and Material BattlesДокумент7 страницLIDO - Activism and The Academy Losing The Ideological and Material BattlesGustavo Martins PiccoloОценок пока нет
- Good Findings-Social ExclusionДокумент4 страницыGood Findings-Social ExclusionArasyid GaniОценок пока нет
- Human RightsДокумент22 страницыHuman RightsAiyushiОценок пока нет
- Importance of Interactive Public SpacesДокумент11 страницImportance of Interactive Public SpacesMahima MittalОценок пока нет
- Social Dimension Summary ArnavДокумент12 страницSocial Dimension Summary Arnavarnav saikiaОценок пока нет
- Ethics of Development Induced DisplacementДокумент7 страницEthics of Development Induced DisplacementBushra Khan100% (1)
- Sustainability SlidesДокумент45 страницSustainability SlidesSpaceMui5Оценок пока нет
- Social Constructionism & Social Exclusion: Understanding Marginalized GroupsДокумент35 страницSocial Constructionism & Social Exclusion: Understanding Marginalized GroupssofiaОценок пока нет
- Bfe 10-11Документ1 страницаBfe 10-11Anutosh ChaudhuriОценок пока нет
- C++ QUICK REFERENCE FOR PREPROCESSOR, LITERALS, STATEMENTSДокумент4 страницыC++ QUICK REFERENCE FOR PREPROCESSOR, LITERALS, STATEMENTSgopu65Оценок пока нет
- Optimize site dimensions and floor areas for mixed use developmentДокумент2 страницыOptimize site dimensions and floor areas for mixed use developmentAnutosh ChaudhuriОценок пока нет
- Optimize Land Use With Mixed Development Project LayoutДокумент5 страницOptimize Land Use With Mixed Development Project LayoutAnutosh ChaudhuriОценок пока нет
- Optimization of Areas: Length (M) Area (m2) Value Length (M) Area (m2) ValueДокумент11 страницOptimization of Areas: Length (M) Area (m2) Value Length (M) Area (m2) ValueAnutosh ChaudhuriОценок пока нет
- Nox 1.2Документ42 страницыNox 1.2Anutosh ChaudhuriОценок пока нет
- A C A D I I I: Nutosh Haudhuri 11AR10004 Rchi Tectural ESI GNДокумент1 страницаA C A D I I I: Nutosh Haudhuri 11AR10004 Rchi Tectural ESI GNAnutosh ChaudhuriОценок пока нет
- Evermotion Archmodels Vol.58Документ15 страницEvermotion Archmodels Vol.58Thu Vien Kien TrucОценок пока нет
- ArchOWiz! Problem StatementДокумент4 страницыArchOWiz! Problem StatementAnutosh ChaudhuriОценок пока нет
- Renzo Piano and Richard Rogers' groundbreaking Centre PompidouДокумент24 страницыRenzo Piano and Richard Rogers' groundbreaking Centre PompidouAnutosh Chaudhuri25% (4)
- AAHE Bibo BrochureДокумент16 страницAAHE Bibo BrochureBANGUN RAHMAT TEKNIKОценок пока нет
- Beckman Coulter Allegra X-12 Centrifuge - User ManualДокумент60 страницBeckman Coulter Allegra X-12 Centrifuge - User ManualMohamed Ben MohamedОценок пока нет
- LiftMaster 3585 Owners ManualДокумент40 страницLiftMaster 3585 Owners ManualazaromeroОценок пока нет
- Wenger Maestro Acoustical Shell-TSДокумент4 страницыWenger Maestro Acoustical Shell-TSportatil31Оценок пока нет
- Building Design Standards 5Документ100 страницBuilding Design Standards 5garych72Оценок пока нет
- Particulars/ Item/ Description Quantity Unit Unit Price Cost 1 General Requirements (Mobilization)Документ3 страницыParticulars/ Item/ Description Quantity Unit Unit Price Cost 1 General Requirements (Mobilization)DIANA DIZONОценок пока нет
- 978 1259278211 Scanned PDF Strategic Management Text and Cases 8th EditionДокумент61 страница978 1259278211 Scanned PDF Strategic Management Text and Cases 8th Editionaudrey.walston606100% (44)
- Evolution 200: Low-To Mid-Rise ElevatorДокумент47 страницEvolution 200: Low-To Mid-Rise ElevatorStefan HodanОценок пока нет
- Project Report On Upvc Door/windows FrameДокумент8 страницProject Report On Upvc Door/windows FrameEIRI Board of Consultants and Publishers67% (3)
- Eds 07 3102 Secondary Substation Civil DesignДокумент26 страницEds 07 3102 Secondary Substation Civil DesignUmerfarooq TawriОценок пока нет
- Construction Bill for Proposed Residence and Nurses' QuarterДокумент18 страницConstruction Bill for Proposed Residence and Nurses' QuarterSATYAM BISENОценок пока нет
- Distribution BoardsДокумент8 страницDistribution BoardsZAhad Ali ZafarОценок пока нет
- Hormann Rollmatic Operator Fitting InstructionsДокумент25 страницHormann Rollmatic Operator Fitting InstructionsJuda's LionОценок пока нет
- Dha BC&TP 2020Документ155 страницDha BC&TP 2020Duresham IlyasОценок пока нет
- PAES 409 Agricultural Structures Standard for Milking ParlorsДокумент12 страницPAES 409 Agricultural Structures Standard for Milking Parlorsjoselito dumdumОценок пока нет
- TN Bus Tender India 2022 - TE Irt202899 Nit Technicalspecifications 12m Long 400mm Floorheight Lowfloor Citybus SignedДокумент75 страницTN Bus Tender India 2022 - TE Irt202899 Nit Technicalspecifications 12m Long 400mm Floorheight Lowfloor Citybus SignedDisability Rights AllianceОценок пока нет
- Elevator Catalog EnglishДокумент43 страницыElevator Catalog EnglishmohammadrezaОценок пока нет
- Tata Indigo & Indigo CSДокумент164 страницыTata Indigo & Indigo CSxtempОценок пока нет
- Speeding-Up Building Plan ApprovalsДокумент6 страницSpeeding-Up Building Plan ApprovalsSakrahu TarrasОценок пока нет
- Astm D 4317 - 98 PDFДокумент6 страницAstm D 4317 - 98 PDFAnyiSakuraОценок пока нет
- The Elysian Hyderabad KondapurДокумент10 страницThe Elysian Hyderabad KondapurElysianОценок пока нет
- CAB-4 Cabinets: GeneralДокумент3 страницыCAB-4 Cabinets: Generaleduardo gonzalezavОценок пока нет
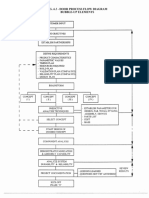
- Door Design Standards and Process Flow DiagramДокумент15 страницDoor Design Standards and Process Flow Diagram김동은Оценок пока нет
- Galvalume Rolling ShuttersДокумент40 страницGalvalume Rolling ShuttersLloyd R. PonceОценок пока нет
- BSD Standard Height and WidthДокумент2 страницыBSD Standard Height and WidthNU EvahОценок пока нет
- Guidelines For Waterless-Double-Chamber Composting Toilets V.1 - HPPB (2018)Документ24 страницыGuidelines For Waterless-Double-Chamber Composting Toilets V.1 - HPPB (2018)HPPBОценок пока нет
- Operating Instructions: 207 D 209 D 307 D 309 D 407 D 409 DДокумент103 страницыOperating Instructions: 207 D 209 D 307 D 309 D 407 D 409 DMega Phono0% (1)
- Stockholm Syndrome Visual Script PDFДокумент47 страницStockholm Syndrome Visual Script PDFgrazzia887924Оценок пока нет
- TopSolid TG Wood Advanced v6 16 Us PDFДокумент131 страницаTopSolid TG Wood Advanced v6 16 Us PDFivan pulgarinОценок пока нет
- Swift BrochureДокумент8 страницSwift BrochureprkushОценок пока нет