Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Orthognathic SurgeryДокумент61 страницаOrthognathic SurgeryVaibhav NagarajОценок пока нет
- Anatomy of Fascial SpacesДокумент68 страницAnatomy of Fascial SpacesVaibhav Nagaraj100% (1)
- Anatomy of Fascial SpacesДокумент68 страницAnatomy of Fascial SpacesVaibhav Nagaraj100% (1)
- Impaction SДокумент127 страницImpaction SVaibhav Nagaraj75% (4)
- Medicalschooltrainingfor Thesurgeon: Christopher P. Scally,, Rebecca M. MinterДокумент13 страницMedicalschooltrainingfor Thesurgeon: Christopher P. Scally,, Rebecca M. MinterDiana C Muñoz VidalОценок пока нет
- Transport of The Critically Ill Patient PDFДокумент4 страницыTransport of The Critically Ill Patient PDFaksinuОценок пока нет
- FINAL Yearbook 2016 Part 6 Health and Applied SciencesДокумент45 страницFINAL Yearbook 2016 Part 6 Health and Applied SciencesDitend TeshОценок пока нет
- Medico-Legal Aspect of InjuryДокумент25 страницMedico-Legal Aspect of InjuryShahriar Shaon100% (1)
- Basic First AidДокумент81 страницаBasic First AidDrVarun Menon100% (1)
- FUNDAMENTALS OF TACTICAL COMBAT CASUALTY CARE For PPSCДокумент80 страницFUNDAMENTALS OF TACTICAL COMBAT CASUALTY CARE For PPSColiver garcianoОценок пока нет
- Emergency Action PrincipleДокумент1 страницаEmergency Action PrincipleJeffrey ViernesОценок пока нет
- FULL Download Ebook PDF International Trauma Life Support For Emergency Care Providers 8th Edition PDF EbookДокумент41 страницаFULL Download Ebook PDF International Trauma Life Support For Emergency Care Providers 8th Edition PDF Ebookcarl.helbling118100% (40)
- Lifepak CR2 AEDДокумент12 страницLifepak CR2 AEDEnerspect Medical SolutionsОценок пока нет
- Ais PDFДокумент3 страницыAis PDFMario BritoОценок пока нет
- Cardio Pulmonary Resuscitation MODULДокумент6 страницCardio Pulmonary Resuscitation MODULRahman Al-kahfi ArdiansyahОценок пока нет
- Model of Care For Paediatric Healthcare Executive SummaryДокумент44 страницыModel of Care For Paediatric Healthcare Executive SummarySergio CurteanОценок пока нет
- NAEMT AMLS CommitteeДокумент2 страницыNAEMT AMLS CommitteeJim ThorntonОценок пока нет
- Algorithm-ACLS CA 200731Документ1 страницаAlgorithm-ACLS CA 200731Hyunsoo EllisОценок пока нет
- Abdominal TraumaДокумент60 страницAbdominal Traumaapi-19916399Оценок пока нет
- 2011 BLS Flowchart Arc - Basic - Life - Support 2011Документ1 страница2011 BLS Flowchart Arc - Basic - Life - Support 2011Brian LeeОценок пока нет
- Abdominal Trauma: Presented By: DR Louza Alnqodi, R3Документ77 страницAbdominal Trauma: Presented By: DR Louza Alnqodi, R3reeves_coolОценок пока нет
- Ambulance Response Protocol DraftДокумент3 страницыAmbulance Response Protocol DraftCommand CenterОценок пока нет
- Cardiopulmonary Resuscitation (CPR) : ImportanceДокумент19 страницCardiopulmonary Resuscitation (CPR) : Importancesxm2901Оценок пока нет
- SCAI Shock Classification DeckДокумент22 страницыSCAI Shock Classification DeckJimmy JimmyОценок пока нет
- 4 - Prehospital Management Particularities of The Patient With Cardiorespiratory ArrestДокумент18 страниц4 - Prehospital Management Particularities of The Patient With Cardiorespiratory ArrestGhimpu DanielaОценок пока нет
- Modes of Ventilation H L en A02 01a NPДокумент55 страницModes of Ventilation H L en A02 01a NPSayan SenОценок пока нет
- Trauma Symposium Program 2019Документ3 страницыTrauma Symposium Program 2019Nick KarundengОценок пока нет
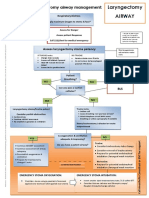
- Laryngectomy Airway: Emergency Tracheostomy Airway ManagementДокумент1 страницаLaryngectomy Airway: Emergency Tracheostomy Airway ManagementDana IlieОценок пока нет
- KINGS Trauma 14Документ138 страницKINGS Trauma 14Shirley SpenceОценок пока нет
- Basic Life Support NSTP 2Документ3 страницыBasic Life Support NSTP 2marymae.mortejoОценок пока нет
- Full Download Emergency Care in Athletic Training 1st Edition Grose Test BankДокумент35 страницFull Download Emergency Care in Athletic Training 1st Edition Grose Test Banksaabatmandearnestus100% (35)
- Dasar Pengelolaan Penderita Gawat Darurat: Dept. Anestesiologi & Terapi Intensif FK-USU/RSUP H.Adam Malik-MedanДокумент47 страницDasar Pengelolaan Penderita Gawat Darurat: Dept. Anestesiologi & Terapi Intensif FK-USU/RSUP H.Adam Malik-Medanfibri fameliaОценок пока нет
- ACLS Skills ChecklistДокумент2 страницыACLS Skills ChecklistabdullahОценок пока нет
- Cardio-Pulmonary Resuscitation: Dr. Sebastian ValceaДокумент16 страницCardio-Pulmonary Resuscitation: Dr. Sebastian ValceaAna MariaОценок пока нет