Вам также может понравиться
- Suspected Neurological Conditions Recognition and Referral PDF 66141663923653Документ76 страницSuspected Neurological Conditions Recognition and Referral PDF 66141663923653Alex GasnasОценок пока нет
- Orofacial Pain - An Update On Diagnosis and Management: PracticeДокумент9 страницOrofacial Pain - An Update On Diagnosis and Management: PracticeAlex GasnasОценок пока нет
- Facial Pain: Neurological and Non-Neurological: Joanna M ZakrzewskaДокумент6 страницFacial Pain: Neurological and Non-Neurological: Joanna M ZakrzewskaAlex GasnasОценок пока нет
- Neuropathic Orofacial Pain Patients in Need of Dental Care: Jcda JadcДокумент7 страницNeuropathic Orofacial Pain Patients in Need of Dental Care: Jcda JadcAlex GasnasОценок пока нет
- Hypoglosal Nerve PalsyДокумент4 страницыHypoglosal Nerve PalsyAlex GasnasОценок пока нет
- MITOCW - MIT9 - 00SCF11 - Lec20 - 300k.mp4: ProfessorДокумент25 страницMITOCW - MIT9 - 00SCF11 - Lec20 - 300k.mp4: ProfessorAlex GasnasОценок пока нет
- Freemasonry Uncovering FreemasonryДокумент113 страницFreemasonry Uncovering Freemasonrycigsas1719100% (1)
- 2150 FullДокумент7 страниц2150 FullAlex GasnasОценок пока нет
- Funke Et Al-2011-The Journal of PhysiologyДокумент13 страницFunke Et Al-2011-The Journal of PhysiologyAlex GasnasОценок пока нет
- Death PathologyДокумент80 страницDeath PathologyAlex GasnasОценок пока нет
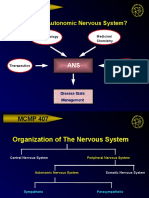
- MCMP 407: Why Study The Autonomic Nervous System?Документ15 страницMCMP 407: Why Study The Autonomic Nervous System?Alex GasnasОценок пока нет
- "Non-Invasive" Brain Stimulation Is Not Non-Invasive: Systems NeuroscienceДокумент4 страницы"Non-Invasive" Brain Stimulation Is Not Non-Invasive: Systems NeuroscienceAlex GasnasОценок пока нет
- Post-Ischemic in Ammation in The Brain: Takashi Shichita, Ryota Sakaguchi, Mayu Suzuki and Akihiko YoshimuraДокумент7 страницPost-Ischemic in Ammation in The Brain: Takashi Shichita, Ryota Sakaguchi, Mayu Suzuki and Akihiko YoshimuraAlex GasnasОценок пока нет
- CNS Other Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaДокумент70 страницCNS Other Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaAlex GasnasОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Director of Major GiftsДокумент2 страницыDirector of Major Giftsapi-78848482Оценок пока нет
- Tricuspid Atresia VivekДокумент66 страницTricuspid Atresia Vivekmihalcea alin100% (1)
- Uporaba Metoda Palijativne Skrbi U Djece Implementation of Palliative Care Methods in ChildrenДокумент7 страницUporaba Metoda Palijativne Skrbi U Djece Implementation of Palliative Care Methods in ChildrenMoonyОценок пока нет
- SEP. 2015 RECALLS MRCOG P2 DR HAMADA Aboromuh PDFДокумент95 страницSEP. 2015 RECALLS MRCOG P2 DR HAMADA Aboromuh PDFuzairОценок пока нет
- Soap NoteДокумент4 страницыSoap Noteapi-252633788100% (7)
- Baxter (Flo-Gard 6201) Volumetric Infusion Pump Flow Rate Accuracy - Test Design and Performance VerificationДокумент21 страницаBaxter (Flo-Gard 6201) Volumetric Infusion Pump Flow Rate Accuracy - Test Design and Performance VerificationKousha TalebianОценок пока нет
- Our Lady of Fatima University College of Medicine Clinical Clerkship Summary of Learning ExperiencesДокумент3 страницыOur Lady of Fatima University College of Medicine Clinical Clerkship Summary of Learning ExperiencesrenzОценок пока нет
- ACTD GuidelinesДокумент18 страницACTD Guidelinesali91Оценок пока нет
- Hubungan Ketepatan Penulisan Informasi Diagnosis Dengan Keakuratan Kode Diagnosis Kasus Obstetry Di Rumah Sakit Umi Barokah BoyolaliДокумент5 страницHubungan Ketepatan Penulisan Informasi Diagnosis Dengan Keakuratan Kode Diagnosis Kasus Obstetry Di Rumah Sakit Umi Barokah BoyolaliirmasariОценок пока нет
- Cerumen Impaction FinalДокумент8 страницCerumen Impaction FinalRose Ann Del MundoОценок пока нет
- Acute Ozone ExposureДокумент2 страницыAcute Ozone ExposurevibhuОценок пока нет
- Disabilities Act 1995Документ4 страницыDisabilities Act 1995directdeoОценок пока нет
- Kulit Emergency in DermatologyДокумент47 страницKulit Emergency in DermatologyAulia Shabrina SyukharialОценок пока нет
- Chapter 10 Syringes and NeedlesДокумент15 страницChapter 10 Syringes and NeedlesTiffany FlorentОценок пока нет
- Vanessa Hoos ResumeДокумент3 страницыVanessa Hoos Resumeapi-533753716Оценок пока нет
- Evidence-Based Practice Fact SheetДокумент3 страницыEvidence-Based Practice Fact Sheetmohamedwhatever100% (2)
- Nandys Principles of Forensic Medicine, 3rd Edition PDFДокумент1 073 страницыNandys Principles of Forensic Medicine, 3rd Edition PDFFahad203693% (14)
- Note On Asthma in AdultДокумент5 страницNote On Asthma in Adultshivam1969Оценок пока нет
- HarveyДокумент6 страницHarveyapi-276953527Оценок пока нет
- Transfusion Checklist Poster June 2021 Ver 1.0 1Документ1 страницаTransfusion Checklist Poster June 2021 Ver 1.0 1Naresh SinghОценок пока нет
- Cara Membaca Foto Thoraks Yang BaikДокумент2 страницыCara Membaca Foto Thoraks Yang BaikIdi Nagan RayaОценок пока нет
- Gambaran Pelaksanaan Kegiatan Program Pengelolaan Penyakit Kronis (Prolanis) Bpjs Kesehatan Di Puskesmas Siak Hulu IIIДокумент10 страницGambaran Pelaksanaan Kegiatan Program Pengelolaan Penyakit Kronis (Prolanis) Bpjs Kesehatan Di Puskesmas Siak Hulu IIIDiky WahyuОценок пока нет
- Proceeding Ilmu KesehatanДокумент183 страницыProceeding Ilmu KesehatanIim Rimba100% (1)
- Malaria DR TariqДокумент32 страницыMalaria DR Tariqdr_hammadОценок пока нет
- NCM 101 Health AssessmentДокумент7 страницNCM 101 Health AssessmentCristoper Bodiongan100% (1)
- Benefits of Living DonationДокумент1 страницаBenefits of Living DonationRanga RajanОценок пока нет
- Xavier BrochureДокумент20 страницXavier BrochureJohn PareraОценок пока нет
- Star Smiley 2007Документ343 страницыStar Smiley 2007David Ajibade100% (1)
- Prevention of Pin Site Infection in External FixatioДокумент11 страницPrevention of Pin Site Infection in External FixatioKim Gabrielle Exene LeeОценок пока нет
- Congenital Postero-Medial Bowing of The Tibia and Fibula: Is Early Surgery Worthwhile?Документ8 страницCongenital Postero-Medial Bowing of The Tibia and Fibula: Is Early Surgery Worthwhile?Kaustubh KeskarОценок пока нет