Вам также может понравиться
- Autacoids: Histamine, Kinins, Serotonin and OndansetronДокумент43 страницыAutacoids: Histamine, Kinins, Serotonin and OndansetronOdiete EfeОценок пока нет
- 9autacoids 14010v9023022 Phpapp02Документ109 страниц9autacoids 14010v9023022 Phpapp02h3cn1r3100% (1)
- Corticosteroids 2 of 2Документ33 страницыCorticosteroids 2 of 2VLDsОценок пока нет
- Pharmacology of Thyroid Hormones and Anti Thyroid Drugs For Second Year Medicine StudentsДокумент48 страницPharmacology of Thyroid Hormones and Anti Thyroid Drugs For Second Year Medicine StudentsAmanuel MaruОценок пока нет
- Pharmacology of The GITДокумент31 страницаPharmacology of The GITmarviecute22Оценок пока нет
- Code of Ethics for Kenyan PharmacistsДокумент20 страницCode of Ethics for Kenyan PharmacistsKevin Chapley50% (2)
- PharmacogeneticsДокумент36 страницPharmacogeneticsAmy YuenОценок пока нет
- Pharmacology - Git DrugsДокумент123 страницыPharmacology - Git DrugsBenjamin Joel Breboneria75% (4)
- Immunomodulators: Drugs that Regulate the Immune SystemДокумент8 страницImmunomodulators: Drugs that Regulate the Immune Systemfaisalnadeem100% (1)
- Problem Based Learning Case Study Thyroid DisorderДокумент30 страницProblem Based Learning Case Study Thyroid DisorderdrnawafОценок пока нет
- RINJUДокумент35 страницRINJUதீபன்குமார் கதிரேசன்100% (1)
- Drugs Affecting Myometrium1 PDFДокумент9 страницDrugs Affecting Myometrium1 PDFЛариса ТкачеваОценок пока нет
- Drugs Interaction1Документ13 страницDrugs Interaction1Akshay MandhotraОценок пока нет
- Amine Autacoids: Histamine & 5-HydroxytryptamineДокумент25 страницAmine Autacoids: Histamine & 5-HydroxytryptamineJames PerianayagamОценок пока нет
- Drug Interaction Can Be Defined As TheДокумент34 страницыDrug Interaction Can Be Defined As TheIstianah Es100% (1)
- Allergy and HypersensitivityДокумент73 страницыAllergy and HypersensitivityAdi PomeranzОценок пока нет
- Thyroid and Antithyroid Agent-VДокумент60 страницThyroid and Antithyroid Agent-VVine100% (1)
- Pharmacology Ain Shams 123 - Compress 1Документ552 страницыPharmacology Ain Shams 123 - Compress 1ahmed hoty100% (1)
- Fluoride Toxicity: Effects, Dosages, TreatmentsДокумент25 страницFluoride Toxicity: Effects, Dosages, TreatmentsNandita KshetrimayumОценок пока нет
- Autocoids and Their AntagonistsДокумент19 страницAutocoids and Their AntagonistsHossein Sehati100% (1)
- Genetic Polymorphism FixДокумент63 страницыGenetic Polymorphism FixBiean gantengОценок пока нет
- Protein Synthesis InhibitorsДокумент25 страницProtein Synthesis InhibitorsSawsan Z. JwaiedОценок пока нет
- Pancreatic Hormones & Antidiabetic DrugsДокумент41 страницаPancreatic Hormones & Antidiabetic DrugsSaddamix AL OmariОценок пока нет
- Receptors and PharmacodynamicsДокумент78 страницReceptors and PharmacodynamicsMuhammad Bilal Bin Amir100% (1)
- Autacoids: Group No. 1Документ92 страницыAutacoids: Group No. 1Rohan Pal100% (1)
- Pharmacology2 (Drug Receptors & Pharmacodynamics)Документ58 страницPharmacology2 (Drug Receptors & Pharmacodynamics)Durge Raj Ghalan100% (2)
- Classification Drugs Acting On GIT. (Lec 1)Документ28 страницClassification Drugs Acting On GIT. (Lec 1)Alee Iz HarОценок пока нет
- Pharmacology: Core Curriculum in NephrologyДокумент11 страницPharmacology: Core Curriculum in NephrologyYuppie RajОценок пока нет
- Basic Pharmacology of Antipsychotic AgentsДокумент29 страницBasic Pharmacology of Antipsychotic AgentsZane PhillipОценок пока нет
- Pharmacology of Pituitary HormonesДокумент54 страницыPharmacology of Pituitary HormonesAmanuel MaruОценок пока нет
- Unit 3 Part 4 Organ-Specific Autoimmune DisordersДокумент23 страницыUnit 3 Part 4 Organ-Specific Autoimmune DisordersReman AlingasaОценок пока нет
- Autacoid PharmacologyДокумент38 страницAutacoid PharmacologyAakkkОценок пока нет
- Immunomodulators: Ma. Stephanie Fay S. Cagayan, MDДокумент67 страницImmunomodulators: Ma. Stephanie Fay S. Cagayan, MDFaye Cagayan100% (1)
- Kasus+gout+dan+hiperuricemiaДокумент3 страницыKasus+gout+dan+hiperuricemiareffadaОценок пока нет
- PCP - Doctors' RightsДокумент26 страницPCP - Doctors' RightsianОценок пока нет
- Bronchodilator & Other Drugs Used in AsthmaДокумент15 страницBronchodilator & Other Drugs Used in AsthmaGenta JagadОценок пока нет
- Geriatric Pharmacotherapy: Understanding Age-Related Changes to Optimize Drug TherapyДокумент48 страницGeriatric Pharmacotherapy: Understanding Age-Related Changes to Optimize Drug Therapywalt65Оценок пока нет
- Pharmacotherapeutics UNIT1Документ44 страницыPharmacotherapeutics UNIT1Bharti ChauhanОценок пока нет
- #3 Pancreatic Hormones & Antidiabetic Drugs 14 PDFДокумент14 страниц#3 Pancreatic Hormones & Antidiabetic Drugs 14 PDFOmar BasimОценок пока нет
- Antiseizures DrugsДокумент27 страницAntiseizures DrugsIrene Zae MwandotoОценок пока нет
- Hormone Receptors and Gene ExpressionДокумент33 страницыHormone Receptors and Gene ExpressionMehwishОценок пока нет
- 2.drugs Acting On The EyeДокумент19 страниц2.drugs Acting On The EyeEman MohamedОценок пока нет
- Pharmacology: Drugs That Affect The: Nervous SystemДокумент84 страницыPharmacology: Drugs That Affect The: Nervous SystemSameh Saber100% (1)
- Case Study - Special Senses and Reproductive SystemДокумент2 страницыCase Study - Special Senses and Reproductive SystemGlydenne Glaire Poncardas GayamОценок пока нет
- RECEPTORSДокумент22 страницыRECEPTORSpharmazone4u100% (1)
- Pharmacotherapeutics 140828123349 Phpapp02Документ14 страницPharmacotherapeutics 140828123349 Phpapp02Anonymous s9i0WyKF200% (1)
- Cholinergic Antagonists "Anticholinergic Drugs" (ParasympatholyticsДокумент32 страницыCholinergic Antagonists "Anticholinergic Drugs" (ParasympatholyticsmiznahОценок пока нет
- Drug InteractionДокумент20 страницDrug InteractionRajendra Moorthy RajendranОценок пока нет
- 6 Beta Adrenergic BlockersДокумент19 страниц6 Beta Adrenergic Blockersmatchees-gone rogue100% (1)
- Contraception and FertilityДокумент11 страницContraception and FertilityWil LesterОценок пока нет
- BiopharmaceuticsДокумент52 страницыBiopharmaceuticsDharma ShantiniОценок пока нет
- Therapeutic Drug Monitoring Guide for Optimal Drug TherapyДокумент13 страницTherapeutic Drug Monitoring Guide for Optimal Drug TherapySujith Kuttan100% (2)
- Cell Wall Inhibitor PPT SlideДокумент47 страницCell Wall Inhibitor PPT Slidekhawaja sahabОценок пока нет
- Hepatotoxicity, Vasculitis:: Pruritic Rash, Arthralgias-Joint Pain, AgranulocytosisДокумент3 страницыHepatotoxicity, Vasculitis:: Pruritic Rash, Arthralgias-Joint Pain, AgranulocytosisThuan Tăng NguyenОценок пока нет
- Autacoids: (Histamine, Serotonin, Eicosanoids, Kinins)Документ31 страницаAutacoids: (Histamine, Serotonin, Eicosanoids, Kinins)Micah MonteОценок пока нет
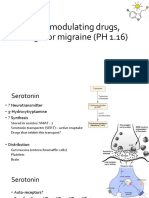
- 5-HT Modulating Drugs, Drugs For Migraine (PH 1.16)Документ13 страниц5-HT Modulating Drugs, Drugs For Migraine (PH 1.16)shruti sangwanОценок пока нет
- VMUF 4 Histamine and Serotonin Antihistaminic Agents Serotonin Modifiers and The Ergot AlkaloidsДокумент29 страницVMUF 4 Histamine and Serotonin Antihistaminic Agents Serotonin Modifiers and The Ergot AlkaloidsSharlene MacaraegОценок пока нет
- Anthistamines 01-11-23Документ35 страницAnthistamines 01-11-23hamzabhayatОценок пока нет
- WHO Dengue Guidelines 2013Документ160 страницWHO Dengue Guidelines 2013Jason MirasolОценок пока нет
- AppendicitisДокумент27 страницAppendicitisnicewanОценок пока нет
- Meds PedsДокумент5 страницMeds PedsnicewanОценок пока нет
- Ebcpg BileductstonesДокумент12 страницEbcpg BileductstonesRatih Lestari UtamiОценок пока нет
- Duchenne Muscular DystrophyДокумент2 страницыDuchenne Muscular DystrophynicewanОценок пока нет
- ROO M General Data Admitt Ing DX Worki NG DX Laboratory Frichmond MedicationsДокумент2 страницыROO M General Data Admitt Ing DX Worki NG DX Laboratory Frichmond MedicationsnicewanОценок пока нет
- FIGO Ovarian Cancer Staging 1.10.14 2Документ2 страницыFIGO Ovarian Cancer Staging 1.10.14 2Elisa Cynthia ArdarickaОценок пока нет
- Intro To ImmunologyДокумент7 страницIntro To ImmunologynicewanОценок пока нет
- Syndromes and DiseasespdfДокумент17 страницSyndromes and DiseasespdfnicewanОценок пока нет
- Lab Flow Sheet Patient MonitoringДокумент2 страницыLab Flow Sheet Patient MonitoringnicewanОценок пока нет
- ACLS Study Guide for IU Health ClassДокумент18 страницACLS Study Guide for IU Health ClassZarah Jane Rull NateОценок пока нет
- Pediatric Care GuideДокумент27 страницPediatric Care GuideFadi AwwadОценок пока нет
- 5 - 1 Diseases of The IntestineДокумент16 страниц5 - 1 Diseases of The IntestinenicewanОценок пока нет
- Ob ReportДокумент37 страницOb ReportnicewanОценок пока нет
- Ten Steps To Successful BreastfeedingДокумент2 страницыTen Steps To Successful BreastfeedingnicewanОценок пока нет
- Infestation SДокумент6 страницInfestation SnicewanОценок пока нет
- San Lazaro Hospital Shifting ExamДокумент6 страницSan Lazaro Hospital Shifting ExamnicewanОценок пока нет
- Cutaneous Drug ReactionsДокумент7 страницCutaneous Drug ReactionsnicewanОценок пока нет
- 5 - 1 Diseases of The IntestineДокумент16 страниц5 - 1 Diseases of The IntestinenicewanОценок пока нет
- 11 13Документ4 страницы11 13nicewanОценок пока нет
- Tetanus CDCДокумент10 страницTetanus CDCZelfi PrimasariОценок пока нет
- Surgery Ortho - TaskДокумент4 страницыSurgery Ortho - TasknicewanОценок пока нет
- OrthopaedicsДокумент3 страницыOrthopaedicsnicewanОценок пока нет
- Cervical Cancer Diagnosis and ManagementДокумент128 страницCervical Cancer Diagnosis and Managementnicewan0% (1)
- Bones of The Upper LimbДокумент8 страницBones of The Upper LimbnicewanОценок пока нет
- Clinical PointsДокумент6 страницClinical PointsnicewanОценок пока нет
- MediastinumДокумент8 страницMediastinumnicewanОценок пока нет
- 2Документ8 страниц2nicewanОценок пока нет
- MediastinumДокумент8 страницMediastinumnicewanОценок пока нет
- 1Документ8 страниц1nicewanОценок пока нет
- 2023Документ25 страниц2023yg hanОценок пока нет
- Food ContaminationДокумент19 страницFood ContaminationAnnelle DabuОценок пока нет
- DAFTAR OBAT DAN PBF (Karunia Farma TGR)Документ2 страницыDAFTAR OBAT DAN PBF (Karunia Farma TGR)mincutttОценок пока нет
- Sumy State University Lecture on AllergiesДокумент56 страницSumy State University Lecture on AllergiesTazrian FarahОценок пока нет
- BIOGENIC AMINE TOXINS IN FOODДокумент4 страницыBIOGENIC AMINE TOXINS IN FOODknaumanОценок пока нет
- Management of Gastric AcidityДокумент23 страницыManagement of Gastric AcidityDharline100% (1)
- PSG 252 Lecture 3 The StomachДокумент5 страницPSG 252 Lecture 3 The StomachMichael TobilobaОценок пока нет
- Slides AUTACOIDSДокумент29 страницSlides AUTACOIDSStrange eeОценок пока нет
- Pharmacology 1.12 Autocoids - Dr. RivadilloДокумент7 страницPharmacology 1.12 Autocoids - Dr. RivadilloAesthetics MinОценок пока нет
- Essential Organic Chemistry (Bruice) Chapter 22 Drug DiscoveryДокумент18 страницEssential Organic Chemistry (Bruice) Chapter 22 Drug Discoverytyron9520Оценок пока нет
- AntihistaminesДокумент4 страницыAntihistaminessharvabhasin0% (1)
- Chemistry in Everyday Life Exercise PDFДокумент8 страницChemistry in Everyday Life Exercise PDFSamridh GuptaОценок пока нет
- The Organic Chemistry of Drugs: Discovery and DesignДокумент17 страницThe Organic Chemistry of Drugs: Discovery and DesignPaul Philip LabitoriaОценок пока нет
- Antihistamine On ChildrenДокумент10 страницAntihistamine On ChildrenOpl OplОценок пока нет
- Morphologic Patterns of Acute InflammationДокумент51 страницаMorphologic Patterns of Acute Inflammationحفصه حسينОценок пока нет
- Antihistamin H2 Struktur-AktivitasДокумент8 страницAntihistamin H2 Struktur-AktivitasNanang Abdul RohmanОценок пока нет
- Anti-Histamines Agents PDFДокумент18 страницAnti-Histamines Agents PDFBintoo SharmaОценок пока нет
- Reactii Adverse Dupa Administrare de IodineДокумент8 страницReactii Adverse Dupa Administrare de IodineahmadОценок пока нет
- Bee Pollen Chemical Composition and Therapeutic ApplicationДокумент6 страницBee Pollen Chemical Composition and Therapeutic ApplicationZeynep Emirhan ŞenyüzОценок пока нет
- Drugs Acting On Functions of Respiratory SystemДокумент73 страницыDrugs Acting On Functions of Respiratory SystemMarin ChianuОценок пока нет
- Histamine Intolerance in Clinical PracticeДокумент9 страницHistamine Intolerance in Clinical PracticeJesse FrontierlandОценок пока нет
- The Allergy Book 1st Edition 2015 PDFДокумент211 страницThe Allergy Book 1st Edition 2015 PDFtuilaai100% (1)
- AntihistaminДокумент46 страницAntihistaminVenerandaОценок пока нет
- 18 - Chemistry in Everyday Life (New) PDFДокумент17 страниц18 - Chemistry in Everyday Life (New) PDFthinkiit60% (10)
- APWCA Synergy Summer Fall 06Документ8 страницAPWCA Synergy Summer Fall 06Krupa ShuklaОценок пока нет
- Allergic Disorder: Dadan Surysaputra 20710031Документ22 страницыAllergic Disorder: Dadan Surysaputra 20710031Dadan SuryasaputraОценок пока нет
- Types of Leucocytes (White Blood Cells) : Lymphocytes: Monocytes: Basophils: Neutrophils: EosinophilsДокумент4 страницыTypes of Leucocytes (White Blood Cells) : Lymphocytes: Monocytes: Basophils: Neutrophils: Eosinophilsjust-maybe202Оценок пока нет
- Chapter 22 Test Bank PatrickДокумент36 страницChapter 22 Test Bank PatrickAmir ali WalizadehОценок пока нет
- Histamine, Serotonin, and Their Antagonists: Classification and Clinical UseДокумент47 страницHistamine, Serotonin, and Their Antagonists: Classification and Clinical Usebangkit99Оценок пока нет
- Autacoids: Definition: Chemical Substances Produced LocallyДокумент23 страницыAutacoids: Definition: Chemical Substances Produced LocallyAlphahin 17Оценок пока нет