Вам также может понравиться
- Test 4 - Coursera PDFДокумент1 страницаTest 4 - Coursera PDFJulian Andres MARTINEZ RINCON20% (10)
- Stop The Bleed 2023Документ22 страницыStop The Bleed 2023Antonio Cáceres Lazo100% (2)
- Fármacos Que Inducen Hemorragia: C. Von Heymann (Modificado Por F. Zaragozá)Документ27 страницFármacos Que Inducen Hemorragia: C. Von Heymann (Modificado Por F. Zaragozá)Jose Carlos Choque MartinesОценок пока нет
- Fondaparinux SpanishДокумент2 страницыFondaparinux SpanishMelissa DelgadoОценок пока нет
- Sistema Nervioso EntericoДокумент14 страницSistema Nervioso EntericoRosyLeyvaОценок пока нет
- La Nueva Ola en HTAДокумент95 страницLa Nueva Ola en HTAMelissa DelgadoОценок пока нет
- Uso Racional de Los Uteroinhibidores en La Practica ClínicaДокумент21 страницаUso Racional de Los Uteroinhibidores en La Practica ClínicaMelissa DelgadoОценок пока нет
- Hallmarks of CancerДокумент23 страницыHallmarks of CancerMelissa DelgadoОценок пока нет
- Revista Iberoamericana de Fertilidad - BuscadorДокумент5 страницRevista Iberoamericana de Fertilidad - BuscadorMelissa DelgadoОценок пока нет
- Los Requerimientos Energéticos Incrementan 12Документ2 страницыLos Requerimientos Energéticos Incrementan 12Melissa DelgadoОценок пока нет
- Fisiologia de La Contracción UterinaДокумент2 страницыFisiologia de La Contracción UterinaMelissa DelgadoОценок пока нет
- Los Requerimientos Energéticos Incrementan 12Документ2 страницыLos Requerimientos Energéticos Incrementan 12Melissa DelgadoОценок пока нет
- Guia Practica Manejo OsteoporosisДокумент73 страницыGuia Practica Manejo OsteoporosisMelissa DelgadoОценок пока нет
- AnginaДокумент18 страницAnginaMelissa DelgadoОценок пока нет
- Guia Practica Manejo OsteoporosisДокумент73 страницыGuia Practica Manejo OsteoporosisMelissa DelgadoОценок пока нет
- GPC Rapida CenetecOsteoporosis020909Документ10 страницGPC Rapida CenetecOsteoporosis020909Natielli SanchezОценок пока нет
- Atlas SpanishДокумент14 страницAtlas SpanishMelissa DelgadoОценок пока нет
- Informe SuicidioДокумент3 страницыInforme SuicidioDiazAlejoPhierinaОценок пока нет
- EMPADRONAMIENTOДокумент26 страницEMPADRONAMIENTOGrober Quispe TerbullinoОценок пока нет
- Etiquetado TareaДокумент3 страницыEtiquetado TareaJazmín JazmiclaОценок пока нет
- ODI para Poda OkДокумент4 страницыODI para Poda Oksebastian andaurОценок пока нет
- Guía de Apoyo para Familiares de Personas Con TEA. Estela Mena JordàДокумент147 страницGuía de Apoyo para Familiares de Personas Con TEA. Estela Mena JordàCarlhos Waliithoo Muñoz Jimenez100% (1)
- NORMAS DEL ISSSTE Elementos Arq. Apoyo DiscapacidadДокумент207 страницNORMAS DEL ISSSTE Elementos Arq. Apoyo DiscapacidadVania VelascoОценок пока нет
- Folleto de EnfermeriaДокумент2 страницыFolleto de EnfermeriaStefany RomeroОценок пока нет
- Trastornos Relacionados Con El DesarrolloДокумент24 страницыTrastornos Relacionados Con El DesarrolloRomeo GonzalezОценок пока нет
- Factor VenusДокумент98 страницFactor VenusGabriel SuarezОценок пока нет
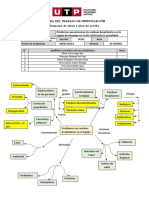
- (AC-S09) Semana 9 - Esquema de Ideas y Plan de AcciónДокумент2 страницы(AC-S09) Semana 9 - Esquema de Ideas y Plan de AcciónJser Misael CsarОценок пока нет
- Evaluación de Actividades 2021-2022Документ16 страницEvaluación de Actividades 2021-2022Mildret Rosales IbarraОценок пока нет
- Trabajo Final de Anatomia Finallll.Документ23 страницыTrabajo Final de Anatomia Finallll.Juan Sebastian Blanquicett AraujoОценок пока нет
- Presentación (43) Emprendimiento Coreano Kawaii Doodling Creativo Marrón PDFДокумент9 страницPresentación (43) Emprendimiento Coreano Kawaii Doodling Creativo Marrón PDFkarlaОценок пока нет
- Ensayo VigorexiaДокумент9 страницEnsayo VigorexiaDavid Gutierrez Ortiz67% (3)
- Listado Estandares Acreditacion ES I-2Документ36 страницListado Estandares Acreditacion ES I-2Dulce MenteОценок пока нет
- Caso 4 - Aplicar Modelo de Mejora ContinuaДокумент11 страницCaso 4 - Aplicar Modelo de Mejora ContinuaLiliana Guerrero ArgoteОценок пока нет
- Seguridad Ocupacional en El Almacén - A&PДокумент11 страницSeguridad Ocupacional en El Almacén - A&PAlexis Osco AlarconОценок пока нет
- Guia de Enfermeria de Administracion de MedicamentosДокумент26 страницGuia de Enfermeria de Administracion de MedicamentosAnsivar Insuasty OrtegaОценок пока нет
- Estres Laboral y Desempeño LaboralДокумент5 страницEstres Laboral y Desempeño LaboralCesar Suarez PaucarОценок пока нет
- Inocuidad Alimentaria FAOДокумент4 страницыInocuidad Alimentaria FAOahiltonОценок пока нет
- Tarea Traumatología UNAHURДокумент2 страницыTarea Traumatología UNAHURMaxi GómezОценок пока нет
- Tratamiento Cognitivo 2018Документ52 страницыTratamiento Cognitivo 2018Ivan Andres TorrisiОценок пока нет
- SA 1 UDA 1 Identificamos Acciones Que Afectan y Fortalecen La Salud EmocionalДокумент3 страницыSA 1 UDA 1 Identificamos Acciones Que Afectan y Fortalecen La Salud EmocionalWIlly EspinozaОценок пока нет
- Historia Clinica ImprimirДокумент5 страницHistoria Clinica ImprimirEdith Paredes CerpaОценок пока нет
- Parkinson - InfografiaДокумент1 страницаParkinson - InfografiaDejavuОценок пока нет
- Síndrome de Ojo Rojo en Atención Primaria: Diagnóstico y ManejoДокумент5 страницSíndrome de Ojo Rojo en Atención Primaria: Diagnóstico y ManejoAlexandra BolivarОценок пока нет
- Quiz 2 2do IntentoДокумент6 страницQuiz 2 2do IntentoAuxiliar Administrativa Consultorio Jurídico DuitamaОценок пока нет
- JRRD 2014 05 0132.en - EsДокумент13 страницJRRD 2014 05 0132.en - EsValentina valencia guerreroОценок пока нет