Вам также может понравиться
- 1 - Factor ViiiДокумент33 страницы1 - Factor ViiiSukma EffendyОценок пока нет
- HemophiliaA Research PaperДокумент7 страницHemophiliaA Research PaperShanePooleОценок пока нет
- Hemophilia AДокумент20 страницHemophilia Adiaharmayukti100% (1)
- Genetics: (Percentage Breakdown of Overall Hemophilia Population by Severity)Документ2 страницыGenetics: (Percentage Breakdown of Overall Hemophilia Population by Severity)uikgykОценок пока нет
- Thalassemia 20-05-2020Документ164 страницыThalassemia 20-05-2020Mohd Anas SheikhОценок пока нет
- Beta Thalassemia: DefinitionДокумент9 страницBeta Thalassemia: Definitioncelestina dawn peterОценок пока нет
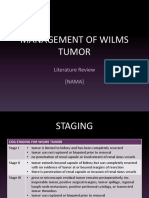
- Management of Wilms Tumor: Literature Review (NAMA)Документ15 страницManagement of Wilms Tumor: Literature Review (NAMA)DeaNataliaОценок пока нет
- ThalassemiaДокумент24 страницыThalassemiaapi-459076195Оценок пока нет
- Coronavirus Disease 2019 (COVID-19) : Because Learning Changes EverythingДокумент29 страницCoronavirus Disease 2019 (COVID-19) : Because Learning Changes EverythingDennis MuthusiОценок пока нет
- ThalassemiaДокумент16 страницThalassemiaAry AffandiОценок пока нет
- Pedia Concepts 2:: From Respiratory Problems To HematologicДокумент119 страницPedia Concepts 2:: From Respiratory Problems To HematologicarudarbmeeОценок пока нет
- Care of Clients With Alterations in Oxygen Carrying Capacity (Hematologic Disorder)Документ30 страницCare of Clients With Alterations in Oxygen Carrying Capacity (Hematologic Disorder)Michael John CanlasОценок пока нет
- Beta Thalassemia: Types Four FormsДокумент8 страницBeta Thalassemia: Types Four FormsAnsu MaliyakalОценок пока нет
- 3M CVP Monitoring - Assisting in BMA ECG Interpretation - Final Draft - 3CДокумент65 страниц3M CVP Monitoring - Assisting in BMA ECG Interpretation - Final Draft - 3CAlexa GoteraОценок пока нет
- High Risk Newborn - Study GuideДокумент10 страницHigh Risk Newborn - Study GuideMalou Yap Buot100% (1)
- Wilms TumorДокумент38 страницWilms TumorEjay Jacob RicamaraОценок пока нет
- Thalassemia TableДокумент2 страницыThalassemia TableMeevie ToledoОценок пока нет
- What Is Covid-19Документ5 страницWhat Is Covid-19Aunia Putri HemasОценок пока нет
- Chapter 28 Summary ThalassemiaДокумент10 страницChapter 28 Summary ThalassemiasanastrikepoОценок пока нет
- Apnea 2019Документ10 страницApnea 2019aiswarya sreekumarОценок пока нет
- Intraventricular Hemorrhage (IVH) : Intensive Care Nursery House Staff ManualДокумент3 страницыIntraventricular Hemorrhage (IVH) : Intensive Care Nursery House Staff Manualjimzz44Оценок пока нет
- Clinician'S Guide: Asthma Management GuidelinesДокумент16 страницClinician'S Guide: Asthma Management GuidelinesNata1511Оценок пока нет
- Commonly Used Drugs in HDДокумент2 страницыCommonly Used Drugs in HDanon_140774008Оценок пока нет
- BLD, Stool, Urine Analysis & MCSДокумент73 страницыBLD, Stool, Urine Analysis & MCSnoblefxОценок пока нет
- What Is CoagulationДокумент6 страницWhat Is CoagulationKang Wenn LeeОценок пока нет
- Anemia in TropicsДокумент7 страницAnemia in TropicsAsnaafii BantiiОценок пока нет
- CestodesДокумент4 страницыCestodesJurel GaoatОценок пока нет
- Blood Products: Product DescriptionДокумент3 страницыBlood Products: Product Descriptionkaychi zОценок пока нет
- Hypertension and Angina DrugsДокумент158 страницHypertension and Angina DrugsMelissa SalayogОценок пока нет
- RESPIRATORY DISORDERS (Abdurahman S)Документ19 страницRESPIRATORY DISORDERS (Abdurahman S)Rahmat MuliaОценок пока нет
- Rheumatic FeverДокумент15 страницRheumatic FeverJeaneta Cheryl PatrickОценок пока нет
- Acute LeukemiaДокумент16 страницAcute Leukemianouval_iqbalОценок пока нет
- Postpartum DisordersДокумент68 страницPostpartum DisordersPrecious SorianoОценок пока нет
- Case Presentation-ChickenpoxДокумент41 страницаCase Presentation-ChickenpoxShaliniОценок пока нет
- Hemophilia AДокумент8 страницHemophilia AroxhencaОценок пока нет
- Hematologic DisordersДокумент32 страницыHematologic DisordersQuolette ConstanteОценок пока нет
- Hemolytic Anemia: MorphologyДокумент10 страницHemolytic Anemia: MorphologyAlya Putri KhairaniОценок пока нет
- CP - Hemophilia 2Документ40 страницCP - Hemophilia 2Reezka PutraОценок пока нет
- Drugs For GUTДокумент11 страницDrugs For GUTAyesha LiaqatОценок пока нет
- Valvular Heart Disease: Aortic Stenosis Aortic Regurgitation Mitral Stenosis Mitral Regurgitation Common EtiologiesДокумент2 страницыValvular Heart Disease: Aortic Stenosis Aortic Regurgitation Mitral Stenosis Mitral Regurgitation Common Etiologiesanisal489Оценок пока нет
- Central Nervous System Infections: Gonzalo B. Roman JR.,MD.,FPSPДокумент72 страницыCentral Nervous System Infections: Gonzalo B. Roman JR.,MD.,FPSPBenjamin PrabhuОценок пока нет
- Lymphoid NeoplasmsДокумент52 страницыLymphoid NeoplasmsAmalia Riska GОценок пока нет
- 7 Dengue FeverДокумент6 страниц7 Dengue FeverNicole HipolОценок пока нет
- Class CestodaДокумент114 страницClass CestodaICAY100% (1)
- Disorders of The Thyroid and Parathyroid Glands: Ms TeamДокумент36 страницDisorders of The Thyroid and Parathyroid Glands: Ms TeamShy Dela PuertaОценок пока нет
- Acute Lymphoblastic LeukemiaДокумент25 страницAcute Lymphoblastic Leukemiaapi-396564080Оценок пока нет
- Transfusion ReactionsДокумент28 страницTransfusion ReactionsRovefrances ErpeluaОценок пока нет
- Acute Post Streptococcal Glomerulonephritis: DiseaseДокумент3 страницыAcute Post Streptococcal Glomerulonephritis: DiseaseHades Luciferos PallonesОценок пока нет
- Nursing Care in AIDSДокумент18 страницNursing Care in AIDSInsaniОценок пока нет
- Hemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUДокумент27 страницHemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUAbdisalan hassanОценок пока нет
- Presentation On ZakahДокумент15 страницPresentation On Zakahhelperforeu50% (2)
- Transfusion Reaction and Coombs Test: Moderator:-Dr Sanjay Agrwal Presenter: - DR Pratima Singh PG Jr-1Документ33 страницыTransfusion Reaction and Coombs Test: Moderator:-Dr Sanjay Agrwal Presenter: - DR Pratima Singh PG Jr-1UmikaguptaОценок пока нет
- Hodgkin's DiseaseДокумент58 страницHodgkin's Diseasealibayaty1Оценок пока нет
- Chronic Myeloid LeukemiaДокумент7 страницChronic Myeloid LeukemiahemendreОценок пока нет
- Von Willebrand Disease PresentДокумент16 страницVon Willebrand Disease PresentPratiba Nair പ്രതിഭ നായര്Оценок пока нет
- EpendymomaДокумент5 страницEpendymomaDenny's BerciaОценок пока нет
- Surgery Papillary Thyroid CAДокумент15 страницSurgery Papillary Thyroid CAMelissa LabadorОценок пока нет
- HEMOPHILIAДокумент70 страницHEMOPHILIAtoyyibОценок пока нет
- Case 1Документ7 страницCase 1secretОценок пока нет
- Increased Intracranial Pressure and Monitoring Site PDFДокумент21 страницаIncreased Intracranial Pressure and Monitoring Site PDFSari RakhmawatiОценок пока нет
- 2 Current Treatment of Dengue Virus InfectionДокумент45 страниц2 Current Treatment of Dengue Virus InfectionSari Rakhmawati100% (1)
- Increased Intracranial Pressure and Monitoring SiteДокумент21 страницаIncreased Intracranial Pressure and Monitoring SiteSari RakhmawatiОценок пока нет
- Thrombolysis Version 2 0 2015 Final PDFДокумент16 страницThrombolysis Version 2 0 2015 Final PDFtitisОценок пока нет
- Antibiotics: Choices For Common InfectionsДокумент30 страницAntibiotics: Choices For Common InfectionsAlfeus GradyОценок пока нет
- Serum Osmolality: Normal 280 - 285mosm Elevated, 285 Mosm Low, 280 MosmДокумент1 страницаSerum Osmolality: Normal 280 - 285mosm Elevated, 285 Mosm Low, 280 MosmSari RakhmawatiОценок пока нет
- Drug Safety AlertДокумент92 страницыDrug Safety AlertFungky AnthonyОценок пока нет
- Increased Intracranial Pressure and Monitoring SiteДокумент21 страницаIncreased Intracranial Pressure and Monitoring SiteSari RakhmawatiОценок пока нет
- Geriatric OtolaryngologyДокумент26 страницGeriatric OtolaryngologySari RakhmawatiОценок пока нет
- Lens CataractДокумент16 страницLens CataractSari RakhmawatiОценок пока нет
- ChemotherapyДокумент21 страницаChemotherapySari RakhmawatiОценок пока нет
- Dr. Yanuar Iman Santosa Sp. THT-KL Dept. THT-KL FK UndipДокумент11 страницDr. Yanuar Iman Santosa Sp. THT-KL Dept. THT-KL FK UndipSari RakhmawatiОценок пока нет
- 3 - Korelasi Antara Derajat Penyakit Sirosis Hati BerdasarkanДокумент13 страниц3 - Korelasi Antara Derajat Penyakit Sirosis Hati BerdasarkanYunita Dwi JayantiОценок пока нет
- DNA DigestionДокумент8 страницDNA DigestionSari RakhmawatiОценок пока нет
- Familial HypercholesterolemiaДокумент7 страницFamilial HypercholesterolemiaSari RakhmawatiОценок пока нет
- Sickle Cell AnemiaДокумент8 страницSickle Cell AnemiaSari RakhmawatiОценок пока нет
- LeukemiaДокумент4 страницыLeukemiaSari RakhmawatiОценок пока нет
- Hypertension Control in African-American Patients With Chronic Kidney DiseaseДокумент3 страницыHypertension Control in African-American Patients With Chronic Kidney Diseaseandikaagus13Оценок пока нет
- Pulmonary Hypertension SymptomsДокумент2 страницыPulmonary Hypertension SymptomsSari RakhmawatiОценок пока нет
- LeukemiaДокумент4 страницыLeukemiaSari RakhmawatiОценок пока нет
- Pulmonary Hypertension SymptomsДокумент2 страницыPulmonary Hypertension SymptomsSari RakhmawatiОценок пока нет
- CIA 5242 Management of Hypertension in The Elderly Patient 092909Документ11 страницCIA 5242 Management of Hypertension in The Elderly Patient 092909Sari RakhmawatiОценок пока нет
- Drug InteractionДокумент11 страницDrug InteractionHubertus Eko BudidharmajaОценок пока нет
- Introduction To PharmacologyДокумент119 страницIntroduction To PharmacologyYzel Vasquez AdavanОценок пока нет
- For Demo in Teaching Strategies by Mike ReyesДокумент10 страницFor Demo in Teaching Strategies by Mike ReyesPaulo Sandino GaliciaОценок пока нет
- ATT Induced Hepatotoxicity: Dr. K. K. SharmaДокумент36 страницATT Induced Hepatotoxicity: Dr. K. K. SharmaSucharita Ray100% (1)
- Essentials in Piezosurger Clinical Advantages in Dentistry VercellottiДокумент136 страницEssentials in Piezosurger Clinical Advantages in Dentistry VercellottiayudewintasariОценок пока нет
- AQA GCSE Separate Science U2 Organisation Knowledge OrganiserДокумент6 страницAQA GCSE Separate Science U2 Organisation Knowledge OrganiserGabriel HoОценок пока нет
- In An Incisional Model of Wound Healing Genistein Aglycone Enhances Skin Recovery A Comparison With Raloxifene and Estradiol in Ovariectomized Rats Is PresentedДокумент10 страницIn An Incisional Model of Wound Healing Genistein Aglycone Enhances Skin Recovery A Comparison With Raloxifene and Estradiol in Ovariectomized Rats Is PresentedAthenaeum Scientific PublishersОценок пока нет
- Journals ListДокумент15 страницJournals ListVanshika JainОценок пока нет
- I Am The CEO of My Own HealthДокумент5 страницI Am The CEO of My Own HealthRoseAnnFloriaОценок пока нет
- Hypertensive Disorders of Pregnancy and AssociatedДокумент10 страницHypertensive Disorders of Pregnancy and AssociatedMedrechEditorialОценок пока нет
- Writing Nurses12 PDFДокумент3 страницыWriting Nurses12 PDFnjОценок пока нет
- Epilepsy and Pregnancy Gynae Course 2013Документ57 страницEpilepsy and Pregnancy Gynae Course 2013Anas KhanОценок пока нет
- Vibitha Joseph Naramvelil: Compassionate - Rehabilitation and Home Care Experience - MultilingualДокумент3 страницыVibitha Joseph Naramvelil: Compassionate - Rehabilitation and Home Care Experience - MultilingualSanish ScariaОценок пока нет
- 4HB0 01 Que 20180110 PDFДокумент28 страниц4HB0 01 Que 20180110 PDFCrustОценок пока нет
- Acute Stress Disorder 1Документ22 страницыAcute Stress Disorder 1Seiska MegaОценок пока нет
- Personal Notes Excpetional StuffДокумент352 страницыPersonal Notes Excpetional StuffYagyeshОценок пока нет
- Anatomi Pembuluh Darah KoronerДокумент36 страницAnatomi Pembuluh Darah KoronerenriОценок пока нет
- Care PlanДокумент2 страницыCare PlanLorina Lynne ApelacioОценок пока нет
- Bowel EliminationДокумент5 страницBowel EliminationDimple Castañeto CalloОценок пока нет
- HyperacusisДокумент5 страницHyperacusisAve FenixОценок пока нет
- Medical Microbiology Made MemorableДокумент113 страницMedical Microbiology Made MemorableParna Praveen90% (10)
- (PDF) Impact of Orthodontic Treatment On Periodontal Tissues A Narrative Review of Multidisciplinary LiteratureДокумент10 страниц(PDF) Impact of Orthodontic Treatment On Periodontal Tissues A Narrative Review of Multidisciplinary LiteratureMirnaLizОценок пока нет
- I Nengah Kundera, Mursito Bialangi: 1. PendahuluanДокумент6 страницI Nengah Kundera, Mursito Bialangi: 1. PendahuluanDesak Putu Widya AprilianiОценок пока нет
- Renal, Urinary Systems - ElectrolytesДокумент692 страницыRenal, Urinary Systems - ElectrolytesRoshan MevadaОценок пока нет
- Diabetes Care in Nigeria - 2015 - Annals of Global Health PDFДокумент9 страницDiabetes Care in Nigeria - 2015 - Annals of Global Health PDFarmanОценок пока нет
- Clinical Experience With Surgical Debridement and Simultaneous Meshed Skin Grafts in Treating Biofilm-Associated Infection: An Exploratory Retrospective Pilot StudyДокумент9 страницClinical Experience With Surgical Debridement and Simultaneous Meshed Skin Grafts in Treating Biofilm-Associated Infection: An Exploratory Retrospective Pilot StudyAsmat BurhanОценок пока нет
- Qso-20-14-Nh - Revised 3-13-2020 PDFДокумент6 страницQso-20-14-Nh - Revised 3-13-2020 PDFAdrian RuxandaОценок пока нет
- CHAPTER 17 - Overview of Human Infectious DiseasesДокумент3 страницыCHAPTER 17 - Overview of Human Infectious DiseasesJacob PallorinaОценок пока нет
- Pre Eclampsia Blood TestДокумент2 страницыPre Eclampsia Blood TestAbhishek RampalОценок пока нет
- GROW VP NB Combined Zs Boys enДокумент2 страницыGROW VP NB Combined Zs Boys enHazel GaringoОценок пока нет
- Chapter7 B and T Cell Activation (1) ImmunologyДокумент21 страницаChapter7 B and T Cell Activation (1) ImmunologyIka BakarОценок пока нет