Вам также может понравиться
- Prof. Dr. Mohamed A. Emam: Mansoura Integrated Fertility Center (MIFC)Документ24 страницыProf. Dr. Mohamed A. Emam: Mansoura Integrated Fertility Center (MIFC)7260678Оценок пока нет
- RECENT ADVANCEMENTS IN INFERTILITY TECHNIQUESДокумент111 страницRECENT ADVANCEMENTS IN INFERTILITY TECHNIQUESsanthanalakshmiОценок пока нет
- Assisted Reproductive TechnologyДокумент12 страницAssisted Reproductive Technologyvpnayak777Оценок пока нет
- In VitrofertilizationДокумент29 страницIn VitrofertilizationRad RYОценок пока нет
- Assisted Reproductive Technology (ART) : and ApplicationДокумент38 страницAssisted Reproductive Technology (ART) : and ApplicationPraluki HerliawanОценок пока нет
- DR Sohani VermaДокумент46 страницDR Sohani VermaKosygin LeishangthemОценок пока нет
- ARTДокумент36 страницARTTtyyfff Fyyu89-Оценок пока нет
- Techniques For Assisted Human ReproductionДокумент51 страницаTechniques For Assisted Human ReproductionArina ChifulescuОценок пока нет
- Assisted Reproductive Technology by Rosemary C. AgboДокумент19 страницAssisted Reproductive Technology by Rosemary C. AgboRosemaryОценок пока нет
- Assisted Reproductive TechnologyДокумент16 страницAssisted Reproductive TechnologyQilaОценок пока нет
- Female Sub FertilityДокумент75 страницFemale Sub FertilityIshaThapaОценок пока нет
- Intrauterine Insemination (IUI)Документ21 страницаIntrauterine Insemination (IUI)Chanta MaharjanОценок пока нет
- Abortion Facts and Laws in NepalДокумент68 страницAbortion Facts and Laws in NepalAasma BidariОценок пока нет
- IVF According to Medico Legal AspecsДокумент20 страницIVF According to Medico Legal AspecslindaОценок пока нет
- Family PlanningДокумент98 страницFamily PlanningDonnaBells Hermo Labaniego50% (2)
- Assisted Reproductive TechniquesДокумент146 страницAssisted Reproductive TechniquesGouravОценок пока нет
- Assisted Reproductive Technologies OverviewДокумент35 страницAssisted Reproductive Technologies OverviewPraluki HerliawanОценок пока нет
- Uterine ProlapseДокумент45 страницUterine ProlapseAnusree AnusreervОценок пока нет
- In The Management of Subfertile Couples: Dr. Jehad Yousef Fics, Frcog Alhayat Art Center Amman - JordanДокумент34 страницыIn The Management of Subfertile Couples: Dr. Jehad Yousef Fics, Frcog Alhayat Art Center Amman - Jordanapi-3771922100% (1)
- Assisted Reproductive TechnologyДокумент14 страницAssisted Reproductive Technologyarchana jainОценок пока нет
- Cne Wad Tingkat 3: Siti Shazwani Binti Zulkaflee RN Ba. Health Sciences (Honor) Nursing, USMДокумент30 страницCne Wad Tingkat 3: Siti Shazwani Binti Zulkaflee RN Ba. Health Sciences (Honor) Nursing, USMWanie Kaflee100% (1)
- Evidence Based Practices in ObstetricsДокумент46 страницEvidence Based Practices in Obstetricsvikas takОценок пока нет
- Embryo TransferДокумент13 страницEmbryo TransferGerwyn Gervacio CОценок пока нет
- Micromanipulation techniquesДокумент6 страницMicromanipulation techniquesSai SridharОценок пока нет
- The Incompetent Cervix 2Документ30 страницThe Incompetent Cervix 2api-3705046100% (3)
- 4 Family Having Difficulty Conceiving A ChildДокумент10 страниц4 Family Having Difficulty Conceiving A ChildDrex CuritanaОценок пока нет
- Assisted ReproductionДокумент22 страницыAssisted ReproductionAbong Che InnocentОценок пока нет
- Assisted Reproductive TechnologyДокумент21 страницаAssisted Reproductive TechnologySurya SetiawanОценок пока нет
- Artificial ReproductionДокумент9 страницArtificial ReproductionSagar HanamasagarОценок пока нет
- EMBRYOLOGY Lab Procedures: Step 1: Evaluation of Female InfertilityДокумент8 страницEMBRYOLOGY Lab Procedures: Step 1: Evaluation of Female InfertilitySaloni KhannaОценок пока нет
- Effect of Reduced Oocyte Aging On The Outcome of Rescue Intracytoplasmic Sperm InjectionДокумент6 страницEffect of Reduced Oocyte Aging On The Outcome of Rescue Intracytoplasmic Sperm InjectiongenesissilvacОценок пока нет
- Embryo Transfer TechnologyДокумент55 страницEmbryo Transfer TechnologyShubham AgrawalОценок пока нет
- Certificate: Abhishek GautamДокумент12 страницCertificate: Abhishek GautamANIL KUMARОценок пока нет
- INFERTILITYДокумент4 страницыINFERTILITYPIH SHTОценок пока нет
- Induction and Augmentation of LaborДокумент22 страницыInduction and Augmentation of LaborDagnachew kasaye100% (1)
- Intrauterine Insemination at Genesis Fertility Center, KalyanДокумент3 страницыIntrauterine Insemination at Genesis Fertility Center, KalyanMayuri SwamiОценок пока нет
- Veterinary ObstericsДокумент50 страницVeterinary ObstericsIbrahim ElkamashОценок пока нет
- IUFDДокумент29 страницIUFDfasyanneshaОценок пока нет
- Obstetric Operations & Procedures2Документ98 страницObstetric Operations & Procedures2mohazemalhotraОценок пока нет
- A Case Presentation: Ectopic PregnancyДокумент10 страницA Case Presentation: Ectopic PregnancyJoshua VillarbaОценок пока нет
- Assisted Reproductive TechnologyДокумент41 страницаAssisted Reproductive Technologyshanty Olivia jasirwanОценок пока нет
- Genitourinary Fistula (VVF) 18066Документ32 страницыGenitourinary Fistula (VVF) 18066Sarvagya ThakurОценок пока нет
- Obstetric FistulaДокумент52 страницыObstetric FistulaAdaiah Priscillia SoibiharryОценок пока нет
- Induction of Labour: A Guide to Methods and ManagementДокумент18 страницInduction of Labour: A Guide to Methods and ManagementNihal ZaidiОценок пока нет
- Anaesthesia For IvfДокумент15 страницAnaesthesia For IvfsequraОценок пока нет
- DR - Asirifi-Induction and Augmentation of Labour (Autosaved)Документ19 страницDR - Asirifi-Induction and Augmentation of Labour (Autosaved)Max ZealОценок пока нет
- Assited Reproductive TechnologyДокумент40 страницAssited Reproductive TechnologySanthosh.S.UОценок пока нет
- Semi Finals CHAPTER IVДокумент5 страницSemi Finals CHAPTER IVjacobprince0016Оценок пока нет
- Artificial Insemination - Docx1Документ3 страницыArtificial Insemination - Docx1carol ann saliseОценок пока нет
- Curs HisteroscopieДокумент105 страницCurs HisteroscopieRaluca HabaОценок пока нет
- Hysterosalpingography /HSG/: By: Ifnan.M /MRTДокумент51 страницаHysterosalpingography /HSG/: By: Ifnan.M /MRTJuhar AhamedОценок пока нет
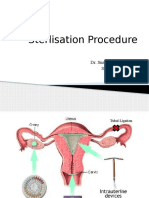
- Sterlisation Procedure: Dr. Sushruta Shrivastava SR Dept of OBGY AIIMS, BhopalДокумент30 страницSterlisation Procedure: Dr. Sushruta Shrivastava SR Dept of OBGY AIIMS, BhopalsushrutaОценок пока нет
- Infertility 2023Документ5 страницInfertility 2023Charlette GuadalupeОценок пока нет
- Fertility AssessmentДокумент38 страницFertility AssessmentSkmc InfertilityОценок пока нет
- Vaginal Birth After Caesarean Section (Vbac)Документ16 страницVaginal Birth After Caesarean Section (Vbac)api-370504650% (2)
- Ectopic Pregnancy: Causes, Symptoms and DiagnosisДокумент60 страницEctopic Pregnancy: Causes, Symptoms and DiagnosisAndrada Doţa100% (1)
- What is oocyte retrievalДокумент20 страницWhat is oocyte retrievalVamsi KrishnaОценок пока нет
- Selecting Male Or Female Child Here's How It Works - Based On The Teachings Of Dr. Andrew Huberman: A Guide To Gender SelectionОт EverandSelecting Male Or Female Child Here's How It Works - Based On The Teachings Of Dr. Andrew Huberman: A Guide To Gender SelectionОценок пока нет
- Gynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenОт EverandGynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenОценок пока нет
- Treatment Strategy for Unexplained Infertility and Recurrent MiscarriageОт EverandTreatment Strategy for Unexplained Infertility and Recurrent MiscarriageKeiji KurodaОценок пока нет
- Benha University Hospital Delta (Mansura) & Benha Fertility CentersДокумент42 страницыBenha University Hospital Delta (Mansura) & Benha Fertility CentersDenisОценок пока нет
- DUB Info For ReportДокумент18 страницDUB Info For ReportDenisОценок пока нет
- LpsДокумент42 страницыLpsDenisОценок пока нет
- IUI ReviewДокумент53 страницыIUI ReviewDenisОценок пока нет
- PCOSДокумент21 страницаPCOSDenisОценок пока нет
- Management of Subfertile Couples Through IUIДокумент34 страницыManagement of Subfertile Couples Through IUIDenis100% (1)
- Investigation InfertilityДокумент44 страницыInvestigation InfertilityDenisОценок пока нет
- Gestatinal Trophoblastic TumorДокумент7 страницGestatinal Trophoblastic TumorDenisОценок пока нет
- IUI PPTBДокумент25 страницIUI PPTBDenisОценок пока нет
- Hymen or Rha PhyДокумент28 страницHymen or Rha PhyDenisОценок пока нет
- Plasma Homocysteine, Fasting Insulin, and Serum Androgens As A Function of Sonographic Ovarian FeaturesДокумент20 страницPlasma Homocysteine, Fasting Insulin, and Serum Androgens As A Function of Sonographic Ovarian FeaturesDenisОценок пока нет
- Transvaginal Sonography and EndometriumДокумент19 страницTransvaginal Sonography and EndometriumDenisОценок пока нет
- Infertility ObgynДокумент33 страницыInfertility ObgynDenisОценок пока нет
- Infertility HysterosДокумент47 страницInfertility HysterosDenisОценок пока нет
- Infertility ObgynДокумент33 страницыInfertility ObgynDenisОценок пока нет
- CloningДокумент80 страницCloningDenisОценок пока нет
- Art of CounselingДокумент10 страницArt of CounselingDenisОценок пока нет
- US Assisted Reproduction Progress Over 20 YearsДокумент15 страницUS Assisted Reproduction Progress Over 20 YearsDenisОценок пока нет
- Infertility HysterosДокумент47 страницInfertility HysterosDenisОценок пока нет
- GN RHДокумент21 страницаGN RHDenisОценок пока нет
- Pcod Natural TreatmentДокумент4 страницыPcod Natural Treatmenttusharphale100% (1)
- NURSING RESEARCH-Questionnaire On Sexually Transmitted InfectionsДокумент3 страницыNURSING RESEARCH-Questionnaire On Sexually Transmitted InfectionsEJ Cubero, R☤NОценок пока нет
- 2011 MARSTON Finding The Balance Jan Kagarice, A Case Study of A Master Trombone TeacherДокумент335 страниц2011 MARSTON Finding The Balance Jan Kagarice, A Case Study of A Master Trombone TeacherRicardo AlvesОценок пока нет
- Spawning Response of African Catfish.... GadisaNateaetal.2017Документ7 страницSpawning Response of African Catfish.... GadisaNateaetal.2017Ardian RahmanОценок пока нет
- Reproductive and FertilisationДокумент22 страницыReproductive and FertilisationRoygunEdwinОценок пока нет
- Obstetrical History and Assessment ActivityДокумент3 страницыObstetrical History and Assessment ActivityNielette R. BASALОценок пока нет
- Blighted Ovum Anembryonic Pregnancy: Mary M. Gallenberg, M.DДокумент4 страницыBlighted Ovum Anembryonic Pregnancy: Mary M. Gallenberg, M.Dadminbunda sehatОценок пока нет
- IVF Process, Fertility Specialist, Ivf Treatment, Cost of IvfДокумент37 страницIVF Process, Fertility Specialist, Ivf Treatment, Cost of IvfBlossom Fertility and IVF CentreОценок пока нет
- Obstetrics and Gynecology Question Papers - Vol IIДокумент19 страницObstetrics and Gynecology Question Papers - Vol IIprinceejОценок пока нет
- Sexual, Marital Perceivednihms199025Документ16 страницSexual, Marital Perceivednihms199025annisa habibullohОценок пока нет
- Family Planning Programs: Monitoring and EvaluationДокумент55 страницFamily Planning Programs: Monitoring and EvaluationRegina HershaaОценок пока нет
- Assited Reproductive TechnologyДокумент40 страницAssited Reproductive TechnologySanthosh.S.UОценок пока нет
- IUD Consent Form ExplainedДокумент2 страницыIUD Consent Form ExplainedShelly PierceОценок пока нет
- Infertility KapДокумент8 страницInfertility Kapmohammadomerkhan96Оценок пока нет
- Progestin-Only Injectables Fact Sheet Final - 102510Документ2 страницыProgestin-Only Injectables Fact Sheet Final - 102510Chan Myae AungОценок пока нет
- Four Types of Social Movements and Their Stages of DevelopmentДокумент19 страницFour Types of Social Movements and Their Stages of DevelopmentQueenielyn TagraОценок пока нет
- Coitus ConsentДокумент3 страницыCoitus ConsentgrondalghoulОценок пока нет
- MCN - Sexuality EtcДокумент29 страницMCN - Sexuality EtcBeatrice ChenОценок пока нет
- GemelliДокумент4 страницыGemellimelatiigdОценок пока нет
- Laboratory Evaluation of InfertilityДокумент8 страницLaboratory Evaluation of InfertilityOndape ValeryОценок пока нет
- Lifestyle and Fertility: The Influence of Stress and Quality of Life On Male FertilityДокумент11 страницLifestyle and Fertility: The Influence of Stress and Quality of Life On Male FertilitySantiago CeliОценок пока нет
- 3rd Summative Test SCIENCE 5Документ3 страницы3rd Summative Test SCIENCE 5Jeje Angeles100% (1)
- Forgotten Transvaginal Cervical Cerclage Stitch in First Pregnancy Benefits Reaped Till The Second PregnancyДокумент2 страницыForgotten Transvaginal Cervical Cerclage Stitch in First Pregnancy Benefits Reaped Till The Second PregnancyAna AdamОценок пока нет
- NSTP Survey Presentation OF CSDP and CBAДокумент14 страницNSTP Survey Presentation OF CSDP and CBAZarina Uadan AvilaОценок пока нет
- FSRH Guideline Emergency Contraception 17mar2017 2Документ65 страницFSRH Guideline Emergency Contraception 17mar2017 2blopper123100% (1)
- Female Reproductive System DiagramsДокумент9 страницFemale Reproductive System DiagramselizabethОценок пока нет
- Effects of Early Pregnancy To StudentsДокумент30 страницEffects of Early Pregnancy To Studentsrejenkaye_0871% (7)
- Relationship Between Ovarian Cyst and InfertilityДокумент7 страницRelationship Between Ovarian Cyst and InfertilityiVriskОценок пока нет
- RIFbookДокумент213 страницRIFbookGaurav S DesaiОценок пока нет
- My Reaction Paper RH Bill (Short)Документ6 страницMy Reaction Paper RH Bill (Short)Arvee Tee Lodronio60% (5)