Вам также может понравиться
- Aturan Minum FitbellyДокумент1 страницаAturan Minum FitbellyTia AriantiОценок пока нет
- Jurnal 4Документ9 страницJurnal 4Tia AriantiОценок пока нет
- Brosur Penyuluhan Gizi Anak SekolahДокумент2 страницыBrosur Penyuluhan Gizi Anak SekolahTia AriantiОценок пока нет
- Jurnal 2Документ9 страницJurnal 2Tia AriantiОценок пока нет
- Jurnal 3Документ10 страницJurnal 3Tia AriantiОценок пока нет
- Jurnal 4Документ9 страницJurnal 4Tia AriantiОценок пока нет
- Daftar PustakaДокумент1 страницаDaftar PustakaTia AriantiОценок пока нет
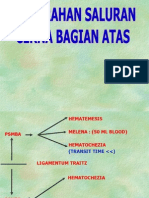
- Perdarahan Saluran Cerna Atas Dan BawahДокумент24 страницыPerdarahan Saluran Cerna Atas Dan BawahTia AriantiОценок пока нет
- 2014 ESC Management of Antithrombotic Therapy in Atrial Fibrillation 1Документ25 страниц2014 ESC Management of Antithrombotic Therapy in Atrial Fibrillation 1Tia AriantiОценок пока нет
- Jurnal 1Документ13 страницJurnal 1Tia AriantiОценок пока нет
- Aids KulДокумент71 страницаAids KulTia AriantiОценок пока нет
- Penyakit Jantung HipertensiДокумент24 страницыPenyakit Jantung HipertensiTia AriantiОценок пока нет
- The Effect of Carvedilol On Morbidity and Mortality in Patients With Heart FaliureДокумент7 страницThe Effect of Carvedilol On Morbidity and Mortality in Patients With Heart Faliurecobby174Оценок пока нет
- Demam 2Документ30 страницDemam 2Tia AriantiОценок пока нет
- PedNas TB 2011-Isi A PDFДокумент59 страницPedNas TB 2011-Isi A PDFYesi SaputriОценок пока нет
- 12-Lead EKG Analysis Fall 20021Документ48 страниц12-Lead EKG Analysis Fall 20021Yesi SaputriОценок пока нет
- Soal Ujian EkgДокумент12 страницSoal Ujian EkgTia AriantiОценок пока нет
- KOLELITIASIS1Документ37 страницKOLELITIASIS1Tia AriantiОценок пока нет
- Demam Tifoid. KulДокумент60 страницDemam Tifoid. KulTia AriantiОценок пока нет
- Falciparum Malaria by DR SarmaДокумент65 страницFalciparum Malaria by DR SarmaTia AriantiОценок пока нет
- Cirrhosis 22008 Bajar Musica Gratis Descargar Musica Gratis Online Descargar Musica Gratis para CelularesДокумент72 страницыCirrhosis 22008 Bajar Musica Gratis Descargar Musica Gratis Online Descargar Musica Gratis para CelularesYeni Chie Aneuk TuleutОценок пока нет
- Hepatic EncephalopathyДокумент16 страницHepatic EncephalopathyTia AriantiОценок пока нет
- 09 Diuretics Upd 2Документ42 страницы09 Diuretics Upd 2Ritari KimyunjongОценок пока нет
- EKG BacaДокумент59 страницEKG BacaTia AriantiОценок пока нет
- Hepatitis (DR - Lukmanhakim Usu)Документ36 страницHepatitis (DR - Lukmanhakim Usu)Tia AriantiОценок пока нет
- Fatty Liver Disease: A Growing EpidemicДокумент31 страницаFatty Liver Disease: A Growing EpidemicTia AriantiОценок пока нет
- RLCirrhosisPortal HTNMunireddy0207Документ41 страницаRLCirrhosisPortal HTNMunireddy0207Tia AriantiОценок пока нет
- Congestive Heart Failure CHF: Nik Nikam, M.DДокумент94 страницыCongestive Heart Failure CHF: Nik Nikam, M.DTia AriantiОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Card 1Документ2 страницыCard 1nalessОценок пока нет
- Pathophysiology of Gestational DMДокумент3 страницыPathophysiology of Gestational DMAnonymous GtR96jCОценок пока нет
- Volume38 - Issue 3 - June Sept 2018Документ107 страницVolume38 - Issue 3 - June Sept 2018wahyulan mОценок пока нет
- Meglitinide Analogues Are Classified As Insulin Secretagogues and Have Actions andДокумент6 страницMeglitinide Analogues Are Classified As Insulin Secretagogues and Have Actions andRifqoh Aulia AlthofunnisaОценок пока нет
- Censo Sospechosos 2017Документ121 страницаCenso Sospechosos 2017KarlaОценок пока нет
- Mild Diabetic Ketoacidosis2Документ10 страницMild Diabetic Ketoacidosis2GorgieОценок пока нет
- 32 PDFДокумент22 страницы32 PDFniallvvОценок пока нет
- Senior Project Research PaperДокумент16 страницSenior Project Research Paperapi-309345535100% (1)
- Diabetic Foot Ulcer Assessment ToolsДокумент16 страницDiabetic Foot Ulcer Assessment ToolsShity Shita ShituОценок пока нет
- Diabetes Care.: Daftar PustakaДокумент3 страницыDiabetes Care.: Daftar PustakaariОценок пока нет
- Presentation 1Документ6 страницPresentation 1Maya RentinaОценок пока нет
- A Comparative Study of Serum Ascorbate Between Newly Diagnosed Type 2 Diabetics and Long Standing Type 2 Diabetics On TreatmentДокумент4 страницыA Comparative Study of Serum Ascorbate Between Newly Diagnosed Type 2 Diabetics and Long Standing Type 2 Diabetics On TreatmentIJAR JOURNALОценок пока нет
- NovorapidДокумент16 страницNovorapidRADITA MAULASARIОценок пока нет
- The Hospital Management of Hypoglycaemia in Adults With Diabetes Mellitus 3rd EditionДокумент40 страницThe Hospital Management of Hypoglycaemia in Adults With Diabetes Mellitus 3rd EditionRumahSehat N-CareОценок пока нет
- Persistence of Islet Autoantibodies After Type 1 Diabetes DiagnosisДокумент7 страницPersistence of Islet Autoantibodies After Type 1 Diabetes DiagnosisrafaelplОценок пока нет
- Interpretation: S03 - FPSC DILSHAD COLONY (C004263143) J-50 Dilshad Colony, DelhiДокумент6 страницInterpretation: S03 - FPSC DILSHAD COLONY (C004263143) J-50 Dilshad Colony, DelhiAll VIDEOS TechОценок пока нет
- Standards of Care in Diabetes-2023: 14. Children and AdolescentsДокумент24 страницыStandards of Care in Diabetes-2023: 14. Children and AdolescentsFranklin MatuteОценок пока нет
- Diabetic Ketoacidosis Case StudyДокумент5 страницDiabetic Ketoacidosis Case Studyjc_albano29100% (7)
- Carolina TrialДокумент59 страницCarolina TrialDr. Abhas ShahОценок пока нет
- Screening of Antidiabetic Drugs: Presented ByДокумент35 страницScreening of Antidiabetic Drugs: Presented BysharonОценок пока нет
- Vol 27 No 1 April 2014 Medicinus 1Документ68 страницVol 27 No 1 April 2014 Medicinus 1Natasya DelarespitaОценок пока нет
- Diabetes The NumbersДокумент24 страницыDiabetes The NumbersSasikala RajendranОценок пока нет
- Handayanijeki@yahoo - Co.id: Ijms - Indonesian Journal On Medical Science - Volume 6 No. 1 - Januari 2019Документ5 страницHandayanijeki@yahoo - Co.id: Ijms - Indonesian Journal On Medical Science - Volume 6 No. 1 - Januari 2019Abu Bilal IbrahimОценок пока нет
- Continuous Glucose Monitoring As A Screening Tool of Neonatal Hypoglycemia in Infant With Diabetic MotherДокумент7 страницContinuous Glucose Monitoring As A Screening Tool of Neonatal Hypoglycemia in Infant With Diabetic MotherraniaulfahОценок пока нет
- Estimation of Blood GlucoseДокумент16 страницEstimation of Blood GlucoseAhmed MohamadОценок пока нет
- South-East Asia Trend P-A M-1 L-12: Number of People Suffering From DM in SEA Region Is Also IncreasingДокумент1 страницаSouth-East Asia Trend P-A M-1 L-12: Number of People Suffering From DM in SEA Region Is Also IncreasingtanzirОценок пока нет
- Anti DiabeticДокумент34 страницыAnti DiabeticEJ GabaoОценок пока нет
- Agency PresentationДокумент17 страницAgency Presentationapi-316466073Оценок пока нет
- DIABETES InfographicДокумент1 страницаDIABETES InfographicDail Xymere YamioОценок пока нет
- Diabetes CCP Slides2Документ72 страницыDiabetes CCP Slides2Pandu WibowoОценок пока нет