Вам также может понравиться
- Tinea Capitis Favus-Like Appearance: Problem of Diagnosis: Dwi Ratna Adisty, Linda AstariДокумент7 страницTinea Capitis Favus-Like Appearance: Problem of Diagnosis: Dwi Ratna Adisty, Linda AstarihaningpradyОценок пока нет
- Fungal Skin Infections-1Документ27 страницFungal Skin Infections-1Fabb Nelson100% (1)
- Detector Vol 1 No 3 Agustus 2023 Hal 223-234Документ12 страницDetector Vol 1 No 3 Agustus 2023 Hal 223-234Shimie Shimie KokobopОценок пока нет
- DERMATOMYCOSISДокумент114 страницDERMATOMYCOSISQonita Qurrota AyunОценок пока нет
- Dermatomycosis Periode 2 Maret - 5 JuniДокумент128 страницDermatomycosis Periode 2 Maret - 5 JuniDevy KurniawatiОценок пока нет
- Tinea Capitis Kerion Type: A Case Report: Laporan KasusДокумент7 страницTinea Capitis Kerion Type: A Case Report: Laporan Kasuswahyu purnamaОценок пока нет
- Fungal InfectionДокумент114 страницFungal InfectionAini Shofa Haniah100% (2)
- Classification and Epidemiology of Communicable DiseasesДокумент40 страницClassification and Epidemiology of Communicable DiseasesRwapembe StephenОценок пока нет
- (JURNAL) Update Terapy MycosesДокумент51 страница(JURNAL) Update Terapy MycosesHabibah Nurla LumiereОценок пока нет
- DR Pankaj Final Paper UploadДокумент5 страницDR Pankaj Final Paper Uploadaman babuОценок пока нет
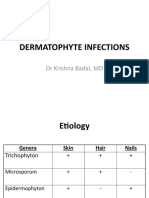
- Dermatophyte InfectionsДокумент41 страницаDermatophyte Infectionsshoaib khanОценок пока нет
- MycologyДокумент55 страницMycologyAlpana Laisom100% (2)
- Eczema: Pathogenesis. Atopic Dermatitis Depends On A Complex Interaction BetweenДокумент5 страницEczema: Pathogenesis. Atopic Dermatitis Depends On A Complex Interaction BetweenSuhas IngaleОценок пока нет
- Dermatophytosis, Chromomycosis and Majocchi's Granuloma: A Review.Документ24 страницыDermatophytosis, Chromomycosis and Majocchi's Granuloma: A Review.Deba P SarmaОценок пока нет
- MycosesДокумент2 страницыMycosesMadabout MusicОценок пока нет
- Role of Homoeopathic Medicines in Tinea Corporis: A Case StudyДокумент4 страницыRole of Homoeopathic Medicines in Tinea Corporis: A Case StudySandip VaghelaОценок пока нет
- Fungal Skin Infections ملزمةДокумент6 страницFungal Skin Infections ملزمةعبدالرحمن طارق عبدالله صالحОценок пока нет
- Fungi of Medical ImportanceДокумент11 страницFungi of Medical ImportanceRi FitrianaОценок пока нет
- Superficial MycosisДокумент30 страницSuperficial MycosisLakshayraj SinghОценок пока нет
- A Clinico-Epidemiological Study On Palmoplantar DermatosesДокумент8 страницA Clinico-Epidemiological Study On Palmoplantar DermatosesIJAR JOURNALОценок пока нет
- Fungal InfectionsДокумент42 страницыFungal InfectionsleenaloveuОценок пока нет
- REFERAT Napkin EzcemaДокумент20 страницREFERAT Napkin Ezcemaade nusrayaОценок пока нет
- CHN Fungal InfectionДокумент14 страницCHN Fungal InfectionChrysteline FabrezОценок пока нет
- Superficial Fungal InfectionДокумент24 страницыSuperficial Fungal InfectionzakiОценок пока нет
- Refer atДокумент4 страницыRefer atArieZta Kautsar RahmanОценок пока нет
- Medical MycologyДокумент14 страницMedical Mycologyhawkar omerОценок пока нет
- Tinea Corporis Pedia-1Документ11 страницTinea Corporis Pedia-1Denso Antonius LimОценок пока нет
- Fungal InfectionsДокумент9 страницFungal InfectionsCoral Srinivasa RamaluОценок пока нет
- Scabies and PediculosisДокумент22 страницыScabies and PediculosisEvady IllusionОценок пока нет
- Case ReportДокумент12 страницCase ReportRimueng GhuenОценок пока нет
- Abstrak RokiДокумент16 страницAbstrak Rokirocky salamaОценок пока нет
- Ringworm (Dermatophytosis)Документ20 страницRingworm (Dermatophytosis)Santosh BhandariОценок пока нет
- Tinea - The DermatophytesДокумент67 страницTinea - The Dermatophytesmansoor aliОценок пока нет
- Novia CASE REPORT KulitДокумент6 страницNovia CASE REPORT KulitNovia ShawolОценок пока нет
- Mycology: Clinical FindingsДокумент5 страницMycology: Clinical FindingsLuqman Al-Bashir FauziОценок пока нет
- Mikosis SuperfisialДокумент46 страницMikosis SuperfisialAdipuraAtmadjaEgokОценок пока нет
- Superficial Fungal Disorders of The SkinДокумент121 страницаSuperficial Fungal Disorders of The SkinhaniОценок пока нет
- Classification of Fungal InfectionsДокумент26 страницClassification of Fungal Infectionstev26100% (1)
- Mycology Lecture FinalДокумент258 страницMycology Lecture FinalBahaa Shaaban100% (1)
- Modul #3 - Student Activity Sheet - CUTANEOUS MYCOSESДокумент7 страницModul #3 - Student Activity Sheet - CUTANEOUS MYCOSESYlia MastarsОценок пока нет
- Fungal InfectionДокумент5 страницFungal InfectionFiras HamidehОценок пока нет
- D.K.M.M. Homoeopathic Medical College & Hospital, AurangabadДокумент14 страницD.K.M.M. Homoeopathic Medical College & Hospital, AurangabadShreyance Parakh100% (1)
- ImpetigoДокумент21 страницаImpetigoHanif GandohОценок пока нет
- Ankur Vashishtha S Ubharti University MeerutДокумент34 страницыAnkur Vashishtha S Ubharti University MeerutKana FajarОценок пока нет
- Superficial Fungal Infections of The Skin VoiceoverДокумент67 страницSuperficial Fungal Infections of The Skin VoiceoverMedo JT100% (1)
- Ourd 20122 26Документ2 страницыOurd 20122 26Armin AbasОценок пока нет
- Tinea CorporisДокумент19 страницTinea CorporisDenny AndreaОценок пока нет
- 6-1 Slideshow MOOC MEMYS GUEGANДокумент14 страниц6-1 Slideshow MOOC MEMYS GUEGANamalОценок пока нет
- The Kerion An Angry Tinea Capitis PBДокумент7 страницThe Kerion An Angry Tinea Capitis PBprajnamitaОценок пока нет
- Kata PengantarДокумент21 страницаKata PengantarKartika RosyahОценок пока нет
- RingwormДокумент7 страницRingwormSAMSON, MAXZENE ANICKAОценок пока нет
- Dermatomycosis 18th July 2021Документ120 страницDermatomycosis 18th July 2021Sekar OktaviaОценок пока нет
- E Tra: Diagnosis and Management of Cutaneous Tinea InfectionsДокумент8 страницE Tra: Diagnosis and Management of Cutaneous Tinea InfectionsFuad hadyanОценок пока нет
- Scabies Guideline Sept 07 PDFДокумент10 страницScabies Guideline Sept 07 PDFMira ApriliaОценок пока нет
- Tinea CapitisДокумент7 страницTinea CapitisNadya LiemОценок пока нет
- SCABIES by DR Pavan PatilДокумент5 страницSCABIES by DR Pavan PatilDr. Pavan PatilОценок пока нет
- Dermatofitosis 2011 1Документ35 страницDermatofitosis 2011 1Carmen Cajina Doña MamiОценок пока нет
- Dermatophytosis: LectureДокумент35 страницDermatophytosis: LectureGideon MukalaziОценок пока нет
- K7 Jamur Superficial 2020Документ51 страницаK7 Jamur Superficial 2020Jimmy Fran IIОценок пока нет
- Data Diagnosa P-CareДокумент458 страницData Diagnosa P-CarerinaОценок пока нет
- Covid19 Reading Comprehension ExercisesДокумент2 страницыCovid19 Reading Comprehension ExercisesMariela SeijasОценок пока нет
- DermatomycosesДокумент34 страницыDermatomycosesRomMy WiEn MicKhoОценок пока нет
- Mtap - Virology NotesДокумент7 страницMtap - Virology NotesMoira Pauline LibroraniaОценок пока нет
- TuberculosisДокумент2 страницыTuberculosisapi-300978388Оценок пока нет
- Basic Facts ON HIV: By: Ms. May Jacklyn C. Radoc-Samson, RN, LPT, MancДокумент20 страницBasic Facts ON HIV: By: Ms. May Jacklyn C. Radoc-Samson, RN, LPT, MancMay Jacklyn RadocОценок пока нет
- FilariaДокумент65 страницFilarialunaghilvin2026Оценок пока нет
- TB - SeminarДокумент12 страницTB - SeminarLaith DmourОценок пока нет
- PoliomyelitisДокумент4 страницыPoliomyelitisapi-3710926100% (2)
- Activity No. 11 Apicomplexan Protozoans I-ObjectivesДокумент2 страницыActivity No. 11 Apicomplexan Protozoans I-ObjectivesCindy NonaОценок пока нет
- Feature ArticleДокумент2 страницыFeature ArticleChantelle BlakeleyОценок пока нет
- Rubella On 22-2-2018Документ48 страницRubella On 22-2-2018farigОценок пока нет
- Hiv/Aids and Stis: ChlamydiaДокумент5 страницHiv/Aids and Stis: Chlamydiaapi-283317714Оценок пока нет
- Faktor-Faktor Predisposisi Yang Berhubungan DenganДокумент13 страницFaktor-Faktor Predisposisi Yang Berhubungan DenganBobozОценок пока нет
- WIFA Recording FormsДокумент96 страницWIFA Recording FormsClaude Ryker TalinioОценок пока нет
- TORCH Infection-2073Документ38 страницTORCH Infection-2073NancyОценок пока нет
- The Black PlagueДокумент3 страницыThe Black PlagueKevin MoralesОценок пока нет
- 01 Diseases - Guess What It IsДокумент11 страниц01 Diseases - Guess What It IsRahmania PamungkasОценок пока нет
- ICD 10 English Indonesia Lengkap 2Документ836 страницICD 10 English Indonesia Lengkap 2DINY NOORKHAYATIОценок пока нет
- Malaria Identification It Is Easier Than You Think!: Susan Flaker Johnson, MT (ASCP), MEPDДокумент30 страницMalaria Identification It Is Easier Than You Think!: Susan Flaker Johnson, MT (ASCP), MEPDasclswisconsinОценок пока нет
- Zika Virus FactsheetДокумент2 страницыZika Virus Factsheetfriska_arianiОценок пока нет
- Communicable Disease ChartДокумент4 страницыCommunicable Disease ChartSanjeev Kumar0% (1)
- Mapeh 8Документ4 страницыMapeh 8Hannah Loth ExceliseОценок пока нет
- CasestudyvaccinesДокумент5 страницCasestudyvaccinesapi-323720899Оценок пока нет
- What Is HIV LBL FДокумент1 страницаWhat Is HIV LBL FKevinОценок пока нет
- Centro Escolar University Makati Campus Department of Nursing 2 SEM 2019-2020 BSN 2asДокумент2 страницыCentro Escolar University Makati Campus Department of Nursing 2 SEM 2019-2020 BSN 2asmyeonnieОценок пока нет
- "Hiv and Aids Awareness of Junior and Senior High School Students" Part I: Profile of RespondentsДокумент1 страница"Hiv and Aids Awareness of Junior and Senior High School Students" Part I: Profile of RespondentsDahl xxОценок пока нет
- Final Exam 2013 Sample Epidemiology of Infectious DiseasesДокумент7 страницFinal Exam 2013 Sample Epidemiology of Infectious DiseasesIsha Bhatt100% (1)
- Powerpoint TaeniasisДокумент23 страницыPowerpoint TaeniasisAyshaShariff0% (1)
- HIVAIDS Crossword Puzzle Answer Key PDFДокумент1 страницаHIVAIDS Crossword Puzzle Answer Key PDFjackie pascualОценок пока нет