Вам также может понравиться
- French DraftДокумент1 страницаFrench Draftmarco_pangilinanОценок пока нет
- AccrualsДокумент2 страницыAccrualsmarco_pangilinanОценок пока нет
- Sophie's World OutlineДокумент23 страницыSophie's World Outlinemarco_pangilinanОценок пока нет
- ThanksДокумент1 страницаThanksmarco_pangilinanОценок пока нет
- ICT StringsДокумент18 страницICT Stringsmarco_pangilinanОценок пока нет
- Automatic Waste SegregatorДокумент7 страницAutomatic Waste SegregatorGanesh Subramanian MohanОценок пока нет
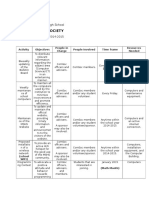
- Computer Society: Manila Science High SchoolДокумент2 страницыComputer Society: Manila Science High Schoolmarco_pangilinanОценок пока нет
- Arts ReviewerДокумент4 страницыArts Reviewermarco_pangilinanОценок пока нет
- FinalictДокумент2 страницыFinalictmarco_pangilinanОценок пока нет
- Tarps SsДокумент3 страницыTarps Ssmarco_pangilinanОценок пока нет
- AdjustmentsДокумент2 страницыAdjustmentsmarco_pangilinanОценок пока нет
- Ict DraftДокумент3 страницыIct Draftmarco_pangilinanОценок пока нет
- Cheese Pastillas: Group 4 9-LinnaeusДокумент7 страницCheese Pastillas: Group 4 9-Linnaeusmarco_pangilinanОценок пока нет
- Measures of Central Tendency: 1 © Mcgraw-Hill, Bluman, 5 Ed, Chapter 3Документ51 страницаMeasures of Central Tendency: 1 © Mcgraw-Hill, Bluman, 5 Ed, Chapter 3marco_pangilinanОценок пока нет
- Statements 1. Reasons Given Definition of PerimeterДокумент2 страницыStatements 1. Reasons Given Definition of Perimetermarco_pangilinanОценок пока нет
- LAYOUTДокумент4 страницыLAYOUTmarco_pangilinanОценок пока нет
- Environmental Science ProjectДокумент7 страницEnvironmental Science Projectmarco_pangilinanОценок пока нет
- GivenДокумент1 страницаGivenmarco_pangilinanОценок пока нет
- Compsci PointersДокумент1 страницаCompsci Pointersmarco_pangilinanОценок пока нет
- Paul Alvinez 3rd Quarter ICT Output 1 ReportДокумент2 страницыPaul Alvinez 3rd Quarter ICT Output 1 Reportmarco_pangilinanОценок пока нет
- ReadmeДокумент1 страницаReadmemarco_pangilinanОценок пока нет
- 36in Trash Bin with Built-In Compactor Promotes SegregationДокумент1 страница36in Trash Bin with Built-In Compactor Promotes Segregationmarco_pangilinanОценок пока нет
- Account Titles PresentationДокумент30 страницAccount Titles Presentationmarco_pangilinanОценок пока нет
- Lemon Citrus Soap: Group 4, 9 - Linnaeus Anos, Pangilinan, Villareal, Cabujat, Erlano, JolejoleДокумент2 страницыLemon Citrus Soap: Group 4, 9 - Linnaeus Anos, Pangilinan, Villareal, Cabujat, Erlano, Jolejolemarco_pangilinanОценок пока нет
- Getting Started - DropboxДокумент6 страницGetting Started - DropboxAnonymous Aeh0aDhF2Оценок пока нет
- Measuring AnglesДокумент2 страницыMeasuring Anglesmarco_pangilinanОценок пока нет
- Marvin James D. Pangilinan, PTRP: Personal InformationДокумент3 страницыMarvin James D. Pangilinan, PTRP: Personal Informationmarco_pangilinanОценок пока нет
- Related LitДокумент4 страницыRelated Litmarco_pangilinanОценок пока нет
- Answer KeyДокумент1 страницаAnswer Keymarco_pangilinanОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Assessing Laura's Substance Abuse Issues and Potential Dual DiagnosesДокумент3 страницыAssessing Laura's Substance Abuse Issues and Potential Dual DiagnosesnylalОценок пока нет
- Early Considerations of Mental IllnessДокумент14 страницEarly Considerations of Mental Illnesszuh blackОценок пока нет
- Anger, Hostility and AggressionДокумент15 страницAnger, Hostility and AggressionJhoe NuevoОценок пока нет
- Mental DisorderДокумент28 страницMental DisorderDaniel CastilloОценок пока нет
- The Divided Self by R D LaingДокумент7 страницThe Divided Self by R D LaingAJITОценок пока нет
- 01 Psychiatric Assessment & DSM-5 BBДокумент62 страницы01 Psychiatric Assessment & DSM-5 BBDhillonvОценок пока нет
- ScriptДокумент12 страницScriptWaleed Nadeem50% (2)
- Abpsy Lecture NotesДокумент10 страницAbpsy Lecture NotesErika BalaniОценок пока нет
- Emetophobia: A Fear of Vomiting: Abhijeet D. Faye, Sushil Gawande, Rahul Tadke, Vivek C. Kirpekar, Sudhir H. BhaveДокумент3 страницыEmetophobia: A Fear of Vomiting: Abhijeet D. Faye, Sushil Gawande, Rahul Tadke, Vivek C. Kirpekar, Sudhir H. Bhavejayadevan vkОценок пока нет
- 2007Документ6 страниц2007api-302133133Оценок пока нет
- Mental Illness BrochureДокумент24 страницыMental Illness BrochureHadley AuliaОценок пока нет
- The Bipolar Affective Disorder Dimension Scale (BADDS) - A Dimensional Scale For Rating Lifetime Psychopathology in Bipolar Spectrum DisordersДокумент11 страницThe Bipolar Affective Disorder Dimension Scale (BADDS) - A Dimensional Scale For Rating Lifetime Psychopathology in Bipolar Spectrum DisordersDM YazdaniОценок пока нет
- Melancholia A Disorder of Movement and Mood A Phenomenological and Neurobiological Review PDFДокумент353 страницыMelancholia A Disorder of Movement and Mood A Phenomenological and Neurobiological Review PDFPer SabОценок пока нет
- Bipolar DisordersДокумент63 страницыBipolar DisorderselvinegunawanОценок пока нет
- The Last Time I Wore A Dress Paper PDFДокумент8 страницThe Last Time I Wore A Dress Paper PDFapi-490648327Оценок пока нет
- Band - Aid SolutionДокумент2 страницыBand - Aid SolutionArhlieJaneEvangelistaОценок пока нет
- DSM-IV-TR Diagnostic System OverviewДокумент26 страницDSM-IV-TR Diagnostic System Overviewanon_4428323320% (1)
- A Case Report On Maladaptive Daydreaming: Key WordsДокумент4 страницыA Case Report On Maladaptive Daydreaming: Key WordsJonathan Quiñonez MoralesОценок пока нет
- Madness by Marya Hornbacher - Discussion QuestionsДокумент3 страницыMadness by Marya Hornbacher - Discussion QuestionsHoughton Mifflin HarcourtОценок пока нет
- Homeopathic Management of Defiant and Violent ChildrenДокумент119 страницHomeopathic Management of Defiant and Violent ChildrenJacqueline Tan100% (10)
- Pediatric Symptom Checklist-17 (PSC-17)Документ1 страницаPediatric Symptom Checklist-17 (PSC-17)Pija RamliОценок пока нет
- Paranoid Schizophrenia.Документ4 страницыParanoid Schizophrenia.Andrada KígyóОценок пока нет
- Hallucinations - Pseudohallucinations and ParahallucinationsДокумент9 страницHallucinations - Pseudohallucinations and ParahallucinationsMas EmmaОценок пока нет
- 3 Sided Essay FinalДокумент3 страницы3 Sided Essay FinalDominique TaylorОценок пока нет
- Scoring Instructions For The Beck Inventories 1Документ2 страницыScoring Instructions For The Beck Inventories 1Philip fred100% (2)
- Delusional Disorder: Molecular Genetic Evidence For Dopamine PsychosisДокумент8 страницDelusional Disorder: Molecular Genetic Evidence For Dopamine PsychosisRadina RusevaОценок пока нет
- RSD: What Is Rejection Sensitive Dysphoria and How Can It Be TreatedДокумент3 страницыRSD: What Is Rejection Sensitive Dysphoria and How Can It Be TreatedDomingo Ignacio100% (3)
- Impulse DisordersДокумент77 страницImpulse DisordersimaОценок пока нет
- ParaphiliasДокумент21 страницаParaphiliasGliza Jane100% (1)
- Anxiety DisordersДокумент42 страницыAnxiety DisordersHazel Marie EchavezОценок пока нет