Вам также может понравиться
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideОт EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideОценок пока нет
- Weaning From The VentilatorДокумент15 страницWeaning From The Ventilatorchadchima100% (1)
- Weaning From Mechanical Ventilation/CCM Board ReviewДокумент55 страницWeaning From Mechanical Ventilation/CCM Board ReviewAzmachamberAzmacareОценок пока нет
- Introduction To Ews (Early Warning Scores) : DR Rachael Lucas Teaching Fellow Focp 2016 at SRHДокумент30 страницIntroduction To Ews (Early Warning Scores) : DR Rachael Lucas Teaching Fellow Focp 2016 at SRHPetros Akin-NibosunОценок пока нет
- SLR Ventilator Weaning Education PresentationДокумент48 страницSLR Ventilator Weaning Education PresentationJR VendeventerОценок пока нет
- Spontaneous Awakening Trial PDFДокумент1 страницаSpontaneous Awakening Trial PDFyonoОценок пока нет
- PHECC Field Guide 2011Документ125 страницPHECC Field Guide 2011Michael B. San JuanОценок пока нет
- Newly Revise Emergency Nursing 1Документ65 страницNewly Revise Emergency Nursing 1Mikee PaningbatanОценок пока нет
- SLR Ventilator Weaning Education PresentationДокумент48 страницSLR Ventilator Weaning Education Presentationfallenczar100% (1)
- Book Reading VentilatorДокумент29 страницBook Reading VentilatorIis Rica MustikaОценок пока нет
- Introduction To The Use of Manchester Triage in Accident and Emergency DobbsДокумент16 страницIntroduction To The Use of Manchester Triage in Accident and Emergency Dobbsrosalyn sugayОценок пока нет
- Trauma Scoring System To Predict Mortality Rate inДокумент20 страницTrauma Scoring System To Predict Mortality Rate inhildawati wahyuningsihОценок пока нет
- Difficult Weaning in COVID 19Документ53 страницыDifficult Weaning in COVID 19rkapatworkОценок пока нет
- Prone StudyДокумент13 страницProne StudySanketNandaniОценок пока нет
- CLRT Final ProjectДокумент28 страницCLRT Final Projectapi-358148089Оценок пока нет
- Doctors OrderДокумент10 страницDoctors OrderJan Mikhail Frasco100% (4)
- SAT SBT ProtocolДокумент11 страницSAT SBT ProtocolI C JОценок пока нет
- PEWS Training IndonesiaДокумент36 страницPEWS Training IndonesiaBbenq Prasetyo100% (1)
- ATI - Adult Medical Surgical NGN B (99 Questions and Answers 2023 - Guarantee A+Документ28 страницATI - Adult Medical Surgical NGN B (99 Questions and Answers 2023 - Guarantee A+denis100% (1)
- NCP 28Документ9 страницNCP 28Leanne Joie Lozano100% (1)
- Bedside Sheets CCTCДокумент11 страницBedside Sheets CCTCNishima SagarОценок пока нет
- Ectopi C PregnancyДокумент28 страницEctopi C PregnancySazzad HossainОценок пока нет
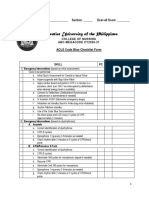
- ABC ACLS Checklist Online CY2020 21Документ8 страницABC ACLS Checklist Online CY2020 21Anastasya Gishella RorongОценок пока нет
- Role Out of Code Blue Team'sДокумент18 страницRole Out of Code Blue Team'sBintang LennyОценок пока нет
- 406 - Respiratory Therapy Consult Service HandbookДокумент28 страниц406 - Respiratory Therapy Consult Service HandbookIkhsan JohnsonОценок пока нет
- Role Out of Code Blue Team'sДокумент18 страницRole Out of Code Blue Team'sBintang Lenny SihotangОценок пока нет
- ACLS PrecourseДокумент7 страницACLS Precoursemohammed ahmedОценок пока нет
- EMR Documentation TemplatesДокумент25 страницEMR Documentation TemplatesFlint Ray100% (1)
- Rapid Response Teams: Aishah Al-Naiem, Omar Quintanar, and Ivan TorresДокумент7 страницRapid Response Teams: Aishah Al-Naiem, Omar Quintanar, and Ivan Torresapi-349065104Оценок пока нет
- Sedation in Critically IllДокумент32 страницыSedation in Critically IllSamantha Deshapriya100% (1)
- Exam 1 Review (PREP) NotesДокумент27 страницExam 1 Review (PREP) Notesmarlen100% (1)
- Rapid Response Teams: Aishah Al-Naiem, Omar Quintanar, and Ivan TorresДокумент7 страницRapid Response Teams: Aishah Al-Naiem, Omar Quintanar, and Ivan Torresapi-348838130Оценок пока нет
- 05 Trauma CareДокумент4 страницы05 Trauma CareKUMUTHA MALAR A/P PARMESWARANОценок пока нет
- Defibrillation Strategies For Refractory Ventricular FibrillationДокумент3 страницыDefibrillation Strategies For Refractory Ventricular FibrillationRurgenciasОценок пока нет
- High Flow Nasal Cannula Oxygen GuidelineДокумент24 страницыHigh Flow Nasal Cannula Oxygen GuidelinekkkssbbОценок пока нет
- PCA and Epidural Presentation Outline 2014Документ10 страницPCA and Epidural Presentation Outline 2014sparticuslives100% (1)
- PEWS Training Slides March2017Документ36 страницPEWS Training Slides March2017Altama L. SidartaОценок пока нет
- Basic Life Suppor T: Monalyn B. La-Ao, RN Glenn Ryan Palao-Ay, RNДокумент37 страницBasic Life Suppor T: Monalyn B. La-Ao, RN Glenn Ryan Palao-Ay, RNMarlon Pilis B CanggatОценок пока нет
- The Occasional Intubator: by DR Minh Le Cong RFDS Cairns, April 2011Документ55 страницThe Occasional Intubator: by DR Minh Le Cong RFDS Cairns, April 2011carlodapОценок пока нет
- Partograph PPT 1Документ55 страницPartograph PPT 1Maria Lejani Terencio100% (1)
- COVID-19 Management of Critical Care Cases PDFДокумент6 страницCOVID-19 Management of Critical Care Cases PDFLubna AliОценок пока нет
- Liver Diseases by SlidesgoДокумент74 страницыLiver Diseases by SlidesgoKennie RamirezОценок пока нет
- Student Refresher CourseДокумент87 страницStudent Refresher CourseRaisa S. MariscalОценок пока нет
- Traumatic Brain Injury 2023Документ17 страницTraumatic Brain Injury 2023Fernando Martinez AguilarОценок пока нет
- ArrestДокумент9 страницArrestBimaIndraОценок пока нет
- Aminoglycoside & Vancomycin: Basic TDMДокумент57 страницAminoglycoside & Vancomycin: Basic TDMft84nzzc92Оценок пока нет
- OSCE Sample Cases 1-2023Документ20 страницOSCE Sample Cases 1-2023caiveuuwhgrjwqxumvОценок пока нет
- Vent ProtocolДокумент15 страницVent Protocolihtisham1Оценок пока нет
- When To Stop CPRДокумент32 страницыWhen To Stop CPRpdccОценок пока нет
- TriageДокумент40 страницTriagemody94546Оценок пока нет
- Non-Operating Room Anesthesia (NORA) : A Beginner's GuideДокумент26 страницNon-Operating Room Anesthesia (NORA) : A Beginner's GuidepaulaОценок пока нет
- A Guide To Performing Quality Assured Diagnostic SpirometryДокумент28 страницA Guide To Performing Quality Assured Diagnostic SpirometryLaura MoiseОценок пока нет
- TOACS With KEYДокумент25 страницTOACS With KEYMehwish MughalОценок пока нет
- Dts Admit SimsДокумент6 страницDts Admit SimsWendy Armstrong FranksОценок пока нет
- Spirometry Importance Performing and Interpretation Case ReportsДокумент149 страницSpirometry Importance Performing and Interpretation Case ReportsAnonymous eZqDZbObRi100% (1)
- DbujДокумент11 страницDbujChristopher ChandlerОценок пока нет
- Intraoperative Neurophysiological Monitoring in Hemifacial Spasm: A Practical GuideОт EverandIntraoperative Neurophysiological Monitoring in Hemifacial Spasm: A Practical GuideОценок пока нет
- Wind Energy Systems (Johnson)Документ449 страницWind Energy Systems (Johnson)Mario Shawn Hayden Jr100% (1)
- Engineering Colleges in PuneДокумент8 страницEngineering Colleges in Punepatel_vicky87Оценок пока нет
- Six Sigma IntroДокумент4 страницыSix Sigma Introsingh.abhi08Оценок пока нет
- Block Diagrams EnotesДокумент7 страницBlock Diagrams Enotespatel_vicky87Оценок пока нет
- Transfer Function (Control Engg)Документ18 страницTransfer Function (Control Engg)patel_vicky87100% (1)
- NC Programming VikДокумент36 страницNC Programming Vikpatel_vicky87Оценок пока нет
- Using Tutorials Tutorial 1in MM Tutorial 1in Inch Tutorial 2Документ55 страницUsing Tutorials Tutorial 1in MM Tutorial 1in Inch Tutorial 2patel_vicky87100% (1)
- Morris Vent SynchДокумент38 страницMorris Vent Synchpatel_vicky87Оценок пока нет
- Safety in Gas Cutting & WeldingДокумент16 страницSafety in Gas Cutting & WeldingMitesh MarvaniyaОценок пока нет
- Newhart TechnologyДокумент37 страницNewhart Technologypatel_vicky87Оценок пока нет
- Forensic ScienceДокумент16 страницForensic Sciencepatel_vicky87100% (1)
- Review Vacuum FinalДокумент17 страницReview Vacuum Finalpatel_vicky87Оценок пока нет
- Pumps Ions ModifiedДокумент20 страницPumps Ions Modifiedpatel_vicky87Оценок пока нет
- (Ebook) Making and Testing Biodiesel Made Using EthanolДокумент23 страницы(Ebook) Making and Testing Biodiesel Made Using EthanolkaamaraajanОценок пока нет
- Pratik Seminar Final 2003Документ19 страницPratik Seminar Final 2003patel_vicky87Оценок пока нет
- 1.design of Camless EngineДокумент94 страницы1.design of Camless EngineMehul JoganiОценок пока нет
- A Journey in Self Discovery John HarricharanДокумент193 страницыA Journey in Self Discovery John Harricharanlindalein100% (1)
- NumerologieДокумент22 страницыNumerologieJared Powell100% (1)
- Nanotechnology ApplicationsДокумент11 страницNanotechnology ApplicationsDivya DivyachilaОценок пока нет
- Department of Mechanical EnginneringДокумент11 страницDepartment of Mechanical EnginneringViraj SukaleОценок пока нет
- Substation Battery ChargerДокумент2 страницыSubstation Battery Chargercadtil0% (1)
- Chapter 13 Managerial AccountingДокумент168 страницChapter 13 Managerial AccountingChandler Schleifs100% (4)
- DPWH ReviewerДокумент597 страницDPWH Reviewercharles sedigoОценок пока нет
- Emerging Therapeutic Options in The Management of Diabetes Recent Trends, Challenges and Future DirectionsДокумент21 страницаEmerging Therapeutic Options in The Management of Diabetes Recent Trends, Challenges and Future DirectionsGabriela PachecoОценок пока нет
- Electro-Mechanical SectorДокумент22 страницыElectro-Mechanical SectorKen LeeОценок пока нет
- AVEVA E3D Tutorial Equipment Modeling With Practical ExampleДокумент8 страницAVEVA E3D Tutorial Equipment Modeling With Practical ExampleRamon Alejandro Porras Hernandez100% (1)
- Food ProductionДокумент106 страницFood ProductionAna Marie100% (1)
- Pastor O. I. Kirk, SR D.D LIFE Celebration BookДокумент63 страницыPastor O. I. Kirk, SR D.D LIFE Celebration Booklindakirk1100% (1)
- 2006 - Dong Et Al - Bulk and Dispersed Aqueous Phase Behavior of PhytantriolДокумент7 страниц2006 - Dong Et Al - Bulk and Dispersed Aqueous Phase Behavior of PhytantriolHe ZeeОценок пока нет
- N Methylpyrrolidone: Chemical Synonym General InformationДокумент5 страницN Methylpyrrolidone: Chemical Synonym General InformationMohamed AdelОценок пока нет
- 12.1 ANSYS CompositePrepPostДокумент2 страницы12.1 ANSYS CompositePrepPostLakmal ArandaraОценок пока нет
- Fuk SecДокумент1 страницаFuk SecHirushan MenukaОценок пока нет
- TamasДокумент180 страницTamaslike 2Оценок пока нет
- Annual Syllabus Class 7 1Документ3 страницыAnnual Syllabus Class 7 1Ni shОценок пока нет
- Motion of A Simple Pendulum in A FluidДокумент16 страницMotion of A Simple Pendulum in A FluidGokul JeevaОценок пока нет
- Dyson - Environmental AssesmentДокумент16 страницDyson - Environmental AssesmentShaneWilson100% (5)
- BFE II ScenariosДокумент25 страницBFE II Scenarioselmitxel100% (1)
- MPI Report 009 Sub Structure B668Документ1 страницаMPI Report 009 Sub Structure B668John DolanОценок пока нет
- Macedonian KavalДокумент1 страницаMacedonian Kavalmikiszekely1362Оценок пока нет
- NSTM.512v0.FANS.S9086 RS STM 010 CH 512R21Sep99Документ60 страницNSTM.512v0.FANS.S9086 RS STM 010 CH 512R21Sep99jwfqcw74mfОценок пока нет
- Tools, Equipment, and ParaphernaliaДокумент35 страницTools, Equipment, and Paraphernaliajahnis lopez100% (1)
- Cracked Tooth Syndrome. Part 1 Aetiology and DiagnosisДокумент17 страницCracked Tooth Syndrome. Part 1 Aetiology and Diagnosisfloressam2000Оценок пока нет
- Sop Toh Engine PT MarminДокумент5 страницSop Toh Engine PT MarminBeni WantaraОценок пока нет
- OKM 54MP FlyerДокумент1 страницаOKM 54MP FlyerJohnsonОценок пока нет
- 2014-2015+M70 Retro+Manual+Документ93 страницы2014-2015+M70 Retro+Manual+Bass is heavyОценок пока нет
- PPP-B-676 e PDFДокумент34 страницыPPP-B-676 e PDFffincher4203Оценок пока нет
- Proposal Form NagДокумент1 страницаProposal Form Nagnitheesh kumarОценок пока нет