Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Linux For Beginners - Shane BlackДокумент165 страницLinux For Beginners - Shane BlackQuod Antichristus100% (1)
- Form16 2018 2019Документ10 страницForm16 2018 2019LogeshwaranОценок пока нет
- Photon Trading - Market Structure BasicsДокумент11 страницPhoton Trading - Market Structure Basicstula amar100% (2)
- Condition Monitoring of Steam Turbines by Performance AnalysisДокумент25 страницCondition Monitoring of Steam Turbines by Performance Analysisabuhurairaqazi100% (1)
- 450i User ManualДокумент54 страницы450i User ManualThượng Lê Văn0% (2)
- Guide To Growing MangoДокумент8 страницGuide To Growing MangoRhenn Las100% (2)
- ACIS - Auditing Computer Information SystemДокумент10 страницACIS - Auditing Computer Information SystemErwin Labayog MedinaОценок пока нет
- Hotel Reservation SystemДокумент36 страницHotel Reservation SystemSowmi DaaluОценок пока нет
- Kehamilan Dengan Bekas Sectio Cecar: Disusun Oleh: Heru Maranata Nababan Pembimbing: Dr. Dr. Donel S, Spog (K)Документ36 страницKehamilan Dengan Bekas Sectio Cecar: Disusun Oleh: Heru Maranata Nababan Pembimbing: Dr. Dr. Donel S, Spog (K)Heru Maranata Nababan100% (1)
- Chapter1 Preterm WhoДокумент9 страницChapter1 Preterm WhoHeru Maranata NababanОценок пока нет
- Brady PEA AsystoleДокумент10 страницBrady PEA AsystoleHeru Maranata NababanОценок пока нет
- Acute Pulmonary Edema, Hypotension, ShockДокумент4 страницыAcute Pulmonary Edema, Hypotension, ShockHeru Maranata NababanОценок пока нет
- Specialty Arc Fusion Splicer: FSM-100 SeriesДокумент193 страницыSpecialty Arc Fusion Splicer: FSM-100 SeriesSFTB SoundsFromTheBirdsОценок пока нет
- Aitt Feb 2017 TH Sem IIIДокумент6 страницAitt Feb 2017 TH Sem IIIMadhu KumarОценок пока нет
- Selvan CVДокумент4 страницыSelvan CVsuman_civilОценок пока нет
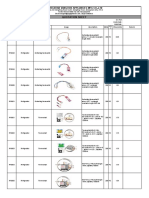
- Vangood Quotation - Refrigerator Part - 2023.3.2Документ5 страницVangood Quotation - Refrigerator Part - 2023.3.2Enmanuel Jossue Artigas VillaОценок пока нет
- Production - The Heart of Organization - TBDДокумент14 страницProduction - The Heart of Organization - TBDSakshi G AwasthiОценок пока нет
- 2016 066 RC - LuelcoДокумент11 страниц2016 066 RC - LuelcoJoshua GatumbatoОценок пока нет
- Properties of Moist AirДокумент11 страницProperties of Moist AirKarthik HarithОценок пока нет
- Strobostomp HD™ Owner'S Instruction Manual V1.1 En: 9V DC Regulated 85maДокумент2 страницыStrobostomp HD™ Owner'S Instruction Manual V1.1 En: 9V DC Regulated 85maShane FairchildОценок пока нет
- Section 8 Illustrations and Parts List: Sullair CorporationДокумент1 страницаSection 8 Illustrations and Parts List: Sullair CorporationBisma MasoodОценок пока нет
- Simoreg ErrorДокумент30 страницSimoreg Errorphth411Оценок пока нет
- Pneumatic Fly Ash Conveying0 PDFДокумент1 страницаPneumatic Fly Ash Conveying0 PDFnjc6151Оценок пока нет
- CodebreakerДокумент3 страницыCodebreakerwarrenОценок пока нет
- Oracle Exadata Database Machine X4-2: Features and FactsДокумент17 страницOracle Exadata Database Machine X4-2: Features and FactsGanesh JОценок пока нет
- Uppsc Ae GSДокумент18 страницUppsc Ae GSFUN TUBEОценок пока нет
- CS321 Computer ArchitectureДокумент160 страницCS321 Computer ArchitectureAnurag kumarОценок пока нет
- Continue: Rudolf Bultmann Theology of The New Testament PDFДокумент3 страницыContinue: Rudolf Bultmann Theology of The New Testament PDFpishoi gerges0% (1)
- Lab 6 PicoblazeДокумент6 страницLab 6 PicoblazeMadalin NeaguОценок пока нет
- Cancellation of Deed of Conditional SalДокумент5 страницCancellation of Deed of Conditional SalJohn RositoОценок пока нет
- MOTOR INSURANCE - Two Wheeler Liability Only SCHEDULEДокумент1 страницаMOTOR INSURANCE - Two Wheeler Liability Only SCHEDULESuhail V VОценок пока нет
- Expense Tracking - How Do I Spend My MoneyДокумент2 страницыExpense Tracking - How Do I Spend My MoneyRenata SánchezОценок пока нет
- TSB 120Документ7 страницTSB 120patelpiyushbОценок пока нет
- Section 26 08 13 - Electrical Systems Prefunctional Checklists and Start-UpsДокумент27 страницSection 26 08 13 - Electrical Systems Prefunctional Checklists and Start-UpsMhya Thu UlunОценок пока нет