Вам также может понравиться
- Nursing Diagnosis For DKAДокумент6 страницNursing Diagnosis For DKARhanne Bolante88% (24)
- Nursing Diagnosis Diabetic KetoacidosisДокумент11 страницNursing Diagnosis Diabetic Ketoacidosismonisha50% (4)
- Case Study 3 Diabetes Mellitus Type 1Документ62 страницыCase Study 3 Diabetes Mellitus Type 1HananErekat100% (2)
- 12a Diabetic Emergencies DKA Case StudiesДокумент13 страниц12a Diabetic Emergencies DKA Case StudiesAnonymous yTdBi7100% (1)
- Nursing Care Plan For "Diabetes Mellitus - Diabetic Ketoacidosis"Документ17 страницNursing Care Plan For "Diabetes Mellitus - Diabetic Ketoacidosis"jhonroks97% (36)
- Nursing Care PlanДокумент10 страницNursing Care PlanZerica Andaca83% (6)
- Diabetic Ketoacidosis Case StudyДокумент6 страницDiabetic Ketoacidosis Case StudyJohn AlcantaraОценок пока нет
- Pediatric & Diabetes Case StudyДокумент3 страницыPediatric & Diabetes Case Studydsaitta108100% (2)
- Nursing Care Plan For Diabetes Mellitus Diabetic KetoacidosisДокумент17 страницNursing Care Plan For Diabetes Mellitus Diabetic KetoacidosisJordz Placi100% (2)
- NCS-DM Type 2 For Case PresentationДокумент49 страницNCS-DM Type 2 For Case Presentationadnelg0771% (7)
- DM Case StudyДокумент4 страницыDM Case Studyapi-273276737100% (3)
- Anatomy and Physiology-Liver CirrhosisДокумент2 страницыAnatomy and Physiology-Liver CirrhosisHilmi Ramos100% (3)
- Pathophys of JaundiceДокумент1 страницаPathophys of JaundiceNathan Vince CruzОценок пока нет
- Artisan Pizza and Flatbread in Five Minutes A DayДокумент13 страницArtisan Pizza and Flatbread in Five Minutes A DayMacmillan Publishers60% (5)
- Module 1 - Case in RealityДокумент2 страницыModule 1 - Case in RealityLong Nguyen Bao0% (2)
- Nursing Care Plan "Diabetes"Документ8 страницNursing Care Plan "Diabetes"Senor SeniorОценок пока нет
- CS Diabetic KetoacidosisДокумент11 страницCS Diabetic KetoacidosisMarvin Dela CruzОценок пока нет
- Diabetic Ketoacidosis Case StudyДокумент5 страницDiabetic Ketoacidosis Case Studyjc_albano29100% (7)
- Dka Case StudyДокумент10 страницDka Case Studyapi-238540303Оценок пока нет
- DKA (Diabetic Ketoacidosis)Документ3 страницыDKA (Diabetic Ketoacidosis)Hassan.shehri83% (6)
- Case Study: Diabetic KetoacidosisДокумент66 страницCase Study: Diabetic Ketoacidosisllaychin100% (2)
- KNH 413 Dka Case Study 2Документ15 страницKNH 413 Dka Case Study 2api-301897220100% (1)
- Diabetic KetoacidosisДокумент76 страницDiabetic Ketoacidosisniyigok100% (1)
- Diabetic KetoacidosisДокумент3 страницыDiabetic KetoacidosisJanna FavilaОценок пока нет
- DKAДокумент64 страницыDKAAravindhan Gunasekaran PaediatricianОценок пока нет
- Diabetic Ketoacidosis Case StudyДокумент6 страницDiabetic Ketoacidosis Case StudyHomework Ping100% (2)
- Anatomy and Physiology DMДокумент3 страницыAnatomy and Physiology DMJisel-Apple Bulan100% (3)
- Case Presentation On Diabetic KetoacidosisДокумент50 страницCase Presentation On Diabetic KetoacidosisJoana Marie Gantuangco-MaglinteОценок пока нет
- APN2 Case Study - DKAДокумент25 страницAPN2 Case Study - DKAElizabeth Ho100% (4)
- Diabetic Ketoacidosis Case StudyДокумент5 страницDiabetic Ketoacidosis Case StudyJully GaciasОценок пока нет
- Diabetic KetoacidosisДокумент6 страницDiabetic KetoacidosisRain Catan Gagarra Saquin100% (1)
- Diabetic KetoacidosisДокумент16 страницDiabetic Ketoacidosisjoyshe111100% (2)
- Case Study of Diabetes MellitusДокумент19 страницCase Study of Diabetes Mellituschai delgadoОценок пока нет
- DkaДокумент83 страницыDkaRajaKumar Ponnana100% (1)
- Diabetic Ketoacidosis (Dka)Документ16 страницDiabetic Ketoacidosis (Dka)yazid100% (5)
- DM Case StudyДокумент4 страницыDM Case Studylspearman100% (7)
- Lanjutan NCP DMДокумент14 страницLanjutan NCP DMVera Andri YaniОценок пока нет
- Diabetic Ketoacidosis Written ReportДокумент19 страницDiabetic Ketoacidosis Written ReportEros Victorino100% (2)
- Nursing Care in Patient With Diabetes MellitusДокумент24 страницыNursing Care in Patient With Diabetes Mellitusmira utami ningsih83% (6)
- NCP FVDДокумент2 страницыNCP FVDMarlon AnryОценок пока нет
- Diabetic KetoacidosisДокумент12 страницDiabetic Ketoacidosispolaris_027Оценок пока нет
- Case Study DMДокумент48 страницCase Study DMBenj Villanueva100% (1)
- Hyperosmolar Hyperglycemic Nonketotic Syndrome (HHNS)Документ8 страницHyperosmolar Hyperglycemic Nonketotic Syndrome (HHNS)amiraОценок пока нет
- Case Study Presentation On Diabetic Foot UlcerДокумент61 страницаCase Study Presentation On Diabetic Foot UlcerBindu GC100% (1)
- Diabetic KetoacidosisДокумент22 страницыDiabetic KetoacidosismartinОценок пока нет
- NCP For DM1Документ2 страницыNCP For DM1Pau Hipol MadriagaОценок пока нет
- Case Study DM TYPE IIДокумент16 страницCase Study DM TYPE IIrose_avy200975% (4)
- Nursing Diagnosis Rationale Interventions Rationale EvaluationДокумент2 страницыNursing Diagnosis Rationale Interventions Rationale EvaluationJobie CasipongОценок пока нет
- Chronic Renal FailureДокумент37 страницChronic Renal Failuredorkiebaby100% (10)
- Nursing Care Plan For Myocardial InfarctionДокумент7 страницNursing Care Plan For Myocardial InfarctionjamieboyRN88% (8)
- Diabetic KetoacidosisДокумент41 страницаDiabetic KetoacidosisdenekeОценок пока нет
- Velez College of Nursing F. Ramos Street, Cebu CityДокумент57 страницVelez College of Nursing F. Ramos Street, Cebu Cityinah krizia lagueОценок пока нет
- Case Analysis FinalДокумент29 страницCase Analysis FinalVeyОценок пока нет
- Diabetic Ketoacidosis: Presented by The Students From Roll Numbers 31 - 40Документ20 страницDiabetic Ketoacidosis: Presented by The Students From Roll Numbers 31 - 40HUSSAIN NAZEESHAОценок пока нет
- Diabetic KetoacidosisДокумент14 страницDiabetic KetoacidosisYash RamawatОценок пока нет
- Case PresentationДокумент31 страницаCase PresentationYogaPratayogaMОценок пока нет
- Diabetic KetoacidosisДокумент4 страницыDiabetic KetoacidosisHasan A. AsFourОценок пока нет
- Diabetes Mellitus of The Human Digestive SystemДокумент7 страницDiabetes Mellitus of The Human Digestive SystemCHRISTINE KARENDIОценок пока нет
- DTS Live Birth, PROM Associated With Severe Pre-Eclampsia and Anemia 2 Degree To Acute Blood LossДокумент30 страницDTS Live Birth, PROM Associated With Severe Pre-Eclampsia and Anemia 2 Degree To Acute Blood LossChe LaiОценок пока нет
- DMДокумент76 страницDMrose ann ayala100% (1)
- CaseДокумент7 страницCaseDenny EmiliusОценок пока нет
- Case Study of Gestational Diabetes Mellitus Group 2Документ19 страницCase Study of Gestational Diabetes Mellitus Group 2nicoleОценок пока нет
- Diabetic Ketoacidosis DKA CeuДокумент36 страницDiabetic Ketoacidosis DKA CeuancyoommenОценок пока нет
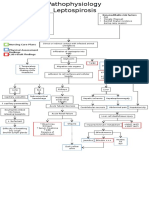
- Pathophysiology LeptospirosisДокумент1 страницаPathophysiology LeptospirosisNathan Vince CruzОценок пока нет
- Modifiable Risk Factors Non-Modifiable Risk Factors: Physical Assessment Findings Lab Result FindingsДокумент1 страницаModifiable Risk Factors Non-Modifiable Risk Factors: Physical Assessment Findings Lab Result FindingsNathan Vince CruzОценок пока нет
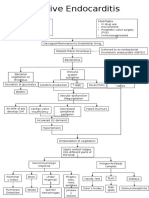
- Infective Endocarditis: Non-Modifiable Age Congenital Heart Disease Gender Preexisting Heart Conditions ModifiableДокумент1 страницаInfective Endocarditis: Non-Modifiable Age Congenital Heart Disease Gender Preexisting Heart Conditions ModifiableNathan Vince CruzОценок пока нет
- Pathophys of UtolethiasisДокумент1 страницаPathophys of UtolethiasisNathan Vince CruzОценок пока нет
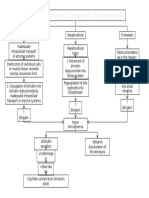
- Pathophysiology CKD Secondary To CGNДокумент1 страницаPathophysiology CKD Secondary To CGNNathan Vince CruzОценок пока нет
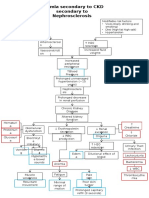
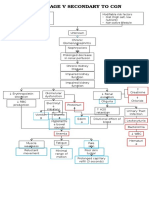
- Pathophysiology Anemia, Secondary To CKD, Secondary To NephrosclerosisДокумент1 страницаPathophysiology Anemia, Secondary To CKD, Secondary To NephrosclerosisNathan Vince CruzОценок пока нет
- Pathophysiology of JaundiceДокумент1 страницаPathophysiology of JaundiceNathan Vince CruzОценок пока нет
- Pathophysiology LeptospirosisДокумент1 страницаPathophysiology LeptospirosisNathan Vince CruzОценок пока нет
- Infective Endocarditis: Non-Modifiable Age Congenital Heart Disease Gender Preexisting Heart Conditions ModifiableДокумент1 страницаInfective Endocarditis: Non-Modifiable Age Congenital Heart Disease Gender Preexisting Heart Conditions ModifiableNathan Vince CruzОценок пока нет
- Pathophysiology Anemia, Secondary To CKD, Secondary To NephrosclerosisДокумент1 страницаPathophysiology Anemia, Secondary To CKD, Secondary To NephrosclerosisNathan Vince CruzОценок пока нет
- Modifiable Risk Factors Non-Modifiable Risk Factors: Physical Assessment Findings Lab Result FindingsДокумент1 страницаModifiable Risk Factors Non-Modifiable Risk Factors: Physical Assessment Findings Lab Result FindingsNathan Vince CruzОценок пока нет
- Pathophys of UtolethiasisДокумент1 страницаPathophys of UtolethiasisNathan Vince CruzОценок пока нет
- Pathophy CKD Secondary To CGNДокумент1 страницаPathophy CKD Secondary To CGNNathan Vince CruzОценок пока нет
- Diabetic Ketoacidosis Case PresentationДокумент37 страницDiabetic Ketoacidosis Case PresentationNathan Vince Cruz100% (2)
- Acute Glumerulo NephritisДокумент13 страницAcute Glumerulo NephritisNathan Vince CruzОценок пока нет
- Business Model and Planning: Vegan Milk Subscription ModelДокумент15 страницBusiness Model and Planning: Vegan Milk Subscription ModelSIDDHANT DAGAОценок пока нет
- CCP and OprpДокумент5 страницCCP and OprpGorack ShirsathОценок пока нет
- List Onboarding BBIДокумент14 страницList Onboarding BBIMiftakhul FaridОценок пока нет
- Street VendorsДокумент26 страницStreet VendorsBharat Bhushan SinghОценок пока нет
- Nestle ProductsДокумент100 страницNestle Productslokesh_045100% (1)
- 49 Shira Barak The Taste of Northern India 2014Документ115 страниц49 Shira Barak The Taste of Northern India 2014Miroslav ĐokićОценок пока нет
- Bathari Menu SEMENTARAДокумент16 страницBathari Menu SEMENTARAamaliska nandaОценок пока нет
- Prevalence and Awareness of Obesity and Its Risk Factors Among Adolescents in Two Schools in A Northeast Indian CityДокумент12 страницPrevalence and Awareness of Obesity and Its Risk Factors Among Adolescents in Two Schools in A Northeast Indian CityShamerra SabtuОценок пока нет
- 1-Pastry Tools and Equipment - 1Документ17 страниц1-Pastry Tools and Equipment - 1Jaswini GanesanОценок пока нет
- Q1 Module 1 For Food and Beverage Services 10 Final MwcisДокумент24 страницыQ1 Module 1 For Food and Beverage Services 10 Final MwcisJames Adrian MiloОценок пока нет
- Vocabulary 5 PlacesДокумент2 страницыVocabulary 5 PlacesELENAОценок пока нет
- TCG Bags The 2018 National Quality Corn Achievers Award: Tuguegarao Named Top 7 Resilient City NationwideДокумент2 страницыTCG Bags The 2018 National Quality Corn Achievers Award: Tuguegarao Named Top 7 Resilient City NationwideJanine Kae UrsulumОценок пока нет
- Term Paper On Pizza HutДокумент8 страницTerm Paper On Pizza Hutaflstjdhs100% (1)
- Potato ThesisДокумент3 страницыPotato ThesisDa VeОценок пока нет
- English Worksheet Unit 4: - Name: - Grade: 3Документ4 страницыEnglish Worksheet Unit 4: - Name: - Grade: 3Coordinacion AcadémicaОценок пока нет
- Gilthead Sea Bream, Sparus Aurata: Life CycleДокумент2 страницыGilthead Sea Bream, Sparus Aurata: Life CycleRiccardoОценок пока нет
- Product ProfileДокумент14 страницProduct ProfilegjrajОценок пока нет
- Blood Biomarkers All Athletes Should KnowДокумент10 страницBlood Biomarkers All Athletes Should KnowkadarzoltanОценок пока нет
- My Melody Planner 2023Документ32 страницыMy Melody Planner 2023Abi Lobato100% (1)
- Winter Holidays Christmas and New Year'S Eve: Christmas or Christmas Day Is AДокумент6 страницWinter Holidays Christmas and New Year'S Eve: Christmas or Christmas Day Is ARoxana Ecaterina ParuschiОценок пока нет
- The Passive To Describe Process Fun Activities Games Grammar Drills 6384Документ2 страницыThe Passive To Describe Process Fun Activities Games Grammar Drills 6384Gayathri Arjunan100% (2)
- Six-Pack Secrets PDFДокумент15 страницSix-Pack Secrets PDFmangozillaОценок пока нет
- OPRP PlanДокумент3 страницыOPRP Plan20125320Оценок пока нет
- Chicken Meat Vs Duck MeatДокумент67 страницChicken Meat Vs Duck Meatsantaanaalfie137Оценок пока нет
- RRL-WPS Office JMДокумент3 страницыRRL-WPS Office JMroyce baeОценок пока нет
- Jewish Standard, August 28, 2015Документ60 страницJewish Standard, August 28, 2015New Jersey Jewish StandardОценок пока нет
- Wind in The Willows AnswersДокумент28 страницWind in The Willows AnswersPiyumi Chathurangi100% (1)
- The Digestive System Summative Test - Q3 - M1Документ2 страницыThe Digestive System Summative Test - Q3 - M1Metchel100% (1)