Вам также может понравиться
- Meningococcal Meningitis - DR Ooi Phaik YeeДокумент66 страницMeningococcal Meningitis - DR Ooi Phaik YeeNg Chee KeongОценок пока нет
- Paediatric Rashes: Ali Faisal SaleemДокумент51 страницаPaediatric Rashes: Ali Faisal Saleemarjumand100% (3)
- DDs of Fever With RashДокумент18 страницDDs of Fever With RashEBОценок пока нет
- Bacterial MeningitisДокумент13 страницBacterial MeningitisJubee FelicianoОценок пока нет
- MeningitisДокумент65 страницMeningitisA. Pathak100% (7)
- Ali - CNS InfectionsДокумент129 страницAli - CNS InfectionsMichael BortzОценок пока нет
- Upper Respıratory Tract InfectıonsДокумент68 страницUpper Respıratory Tract InfectıonsMekdes ZewdeОценок пока нет
- Neonatal MeningitisДокумент10 страницNeonatal MeningitisRana KhairunnisaОценок пока нет
- Infectii Comunitare de Tract Respirator Inferior: AparitiaДокумент14 страницInfectii Comunitare de Tract Respirator Inferior: AparitiaPaul Costas100% (1)
- Presentation On MeningitisДокумент51 страницаPresentation On Meningitissushma shresthaОценок пока нет
- Pigeon Diseases and TreatmentsДокумент1 страницаPigeon Diseases and TreatmentsJohnMasive100% (1)
- Steranios 20 Concentre DS-AEДокумент188 страницSteranios 20 Concentre DS-AEalexa1715Оценок пока нет
- Liofilchem SystemsДокумент12 страницLiofilchem SystemsDialife Medical Equipment and Supplies100% (1)
- MeningitisДокумент34 страницыMeningitispriska maniesОценок пока нет
- Bacterial MeningitisДокумент51 страницаBacterial MeningitiscaseinrenninОценок пока нет
- Clinical Infectious Disease Nplex ReviewДокумент64 страницыClinical Infectious Disease Nplex ReviewValeria AcevedoОценок пока нет
- Approach To The Patient With Fever EditedДокумент72 страницыApproach To The Patient With Fever EditedKevin Karim100% (1)
- Peds - FeverДокумент20 страницPeds - FeverdryogeshrОценок пока нет
- CNS Bacterial Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaДокумент47 страницCNS Bacterial Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaJanPaulaDelaPenaОценок пока нет
- Acute Bacterial MeningitisДокумент40 страницAcute Bacterial Meningitissinte beyuОценок пока нет
- L - 2 - GR (-) CocciДокумент82 страницыL - 2 - GR (-) CocciFahim NadvyОценок пока нет
- Infections of The Eyes and The Central Nervous System - Dr. CerradaДокумент68 страницInfections of The Eyes and The Central Nervous System - Dr. CerradaMonique BorresОценок пока нет
- Pyogenicmeningitis 150928174212 Lva1 App6891Документ45 страницPyogenicmeningitis 150928174212 Lva1 App6891Sri Ram 07Оценок пока нет
- 2011 CNS Bacterial InfectionДокумент47 страниц2011 CNS Bacterial InfectionZEMENAY TRUNEHОценок пока нет
- Kuliah Infeksi SSP 2021Документ85 страницKuliah Infeksi SSP 2021clarissaОценок пока нет
- Infections of The Eyes and The Central Nervous System by Dr. Joan E. CerradaДокумент68 страницInfections of The Eyes and The Central Nervous System by Dr. Joan E. CerradaMonique BorresОценок пока нет
- DNA Viruses 2Документ28 страницDNA Viruses 2sairahhannahОценок пока нет
- TB ConcensusДокумент76 страницTB ConcensusRoxanne Jeen FornollesОценок пока нет
- Viral InfectionДокумент36 страницViral InfectionHani El-asferОценок пока нет
- Peculiarities of Meningitis in ChildrenДокумент6 страницPeculiarities of Meningitis in ChildrenAmalia GeorgiouОценок пока нет
- Sunday Journal - LYMДокумент23 страницыSunday Journal - LYMAlon GoldfainerОценок пока нет
- Enteroviral InfectionsДокумент32 страницыEnteroviral InfectionsTarik PlojovicОценок пока нет
- MeningitisДокумент42 страницыMeningitisRajesh YadavОценок пока нет
- Infections of The Central: Nervous SystemДокумент92 страницыInfections of The Central: Nervous SystemIsabel CastilloОценок пока нет
- Neonatal InfectionsДокумент41 страницаNeonatal Infectionsamid sultanОценок пока нет
- Session 39 MeningitisДокумент25 страницSession 39 MeningitisJohn MoshaОценок пока нет
- Dr. AR - Cns Infection Utk RPSДокумент57 страницDr. AR - Cns Infection Utk RPSKevin KarimОценок пока нет
- CNS Infection DR DPДокумент93 страницыCNS Infection DR DPFini AndrianiОценок пока нет
- Diseases of The Nervous System: Nester 5th. EdДокумент165 страницDiseases of The Nervous System: Nester 5th. EdREBECCA IMPLICAОценок пока нет
- Acute Respiratory Tract InfectionДокумент70 страницAcute Respiratory Tract InfectionCorina OngОценок пока нет
- HFMD N MeningitisДокумент19 страницHFMD N MeningitisNurul AshikinОценок пока нет
- CNS UtiДокумент30 страницCNS UtiArianna MohiuddinОценок пока нет
- Approach To Meningitis and EncephalitisДокумент40 страницApproach To Meningitis and EncephalitisDrvicky BaxiОценок пока нет
- 20 Bacterial MeningitisДокумент35 страниц20 Bacterial MeningitisBhakti WashilkarОценок пока нет
- Acute CNS InfectionsДокумент46 страницAcute CNS InfectionsLily SolОценок пока нет
- Infeksi Susunan Saraf Pusat, Cerebral Palsy DanДокумент64 страницыInfeksi Susunan Saraf Pusat, Cerebral Palsy DanRizky KurniawanОценок пока нет
- Common Cold: Milan Karki 4062Документ20 страницCommon Cold: Milan Karki 4062BinayaОценок пока нет
- Varicella Zooster: Suryadi Susanto Pediatric Department Krida Wacana Christian UniversityДокумент18 страницVaricella Zooster: Suryadi Susanto Pediatric Department Krida Wacana Christian Universitymichelle95Оценок пока нет
- Microbial Diseases of The Nervous System: DR Sonnie P. Talavera 08162009 OlfuДокумент162 страницыMicrobial Diseases of The Nervous System: DR Sonnie P. Talavera 08162009 Olfuone_nd_onlyu0% (1)
- Fiebre Sin FocoДокумент47 страницFiebre Sin FocoTabatha Velarde ValenciaОценок пока нет
- DNA VirusesДокумент99 страницDNA VirusesCourtny Lenz Maygay GapaОценок пока нет
- BB Childhood Diseases Fall12Документ32 страницыBB Childhood Diseases Fall12phoenix180Оценок пока нет
- Viral Meningitis and Aseptic Meningitis Syndrome: Ahmad Rizal Ganiem Dept. Neurology Hasan Sadikin Hospital BandungДокумент15 страницViral Meningitis and Aseptic Meningitis Syndrome: Ahmad Rizal Ganiem Dept. Neurology Hasan Sadikin Hospital BandungYobbi ArissaputraОценок пока нет
- Pathogenesis of MENINGITISДокумент30 страницPathogenesis of MENINGITISPrachi TeteОценок пока нет
- Fever and Rash Mar 2016Документ30 страницFever and Rash Mar 2016almiraerickaiОценок пока нет
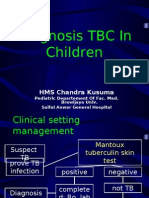
- Diagnosis TBДокумент44 страницыDiagnosis TBGede Eka Putra NugrahaОценок пока нет
- Asuhan Keperawatan Pada Klien Dengan Meningitis: Retno LestariДокумент57 страницAsuhan Keperawatan Pada Klien Dengan Meningitis: Retno Lestariaha ehe ohoОценок пока нет
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingДокумент62 страницыUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingErica Veluz LuyunОценок пока нет
- Sexually Transmitted DiseaseДокумент36 страницSexually Transmitted DiseasesmrutuОценок пока нет
- CNS Infections - MeningitisДокумент156 страницCNS Infections - MeningitisauОценок пока нет
- Meningitis PLUS: Goetz: Textbook of Clinical Neurology, 1st EdДокумент1 страницаMeningitis PLUS: Goetz: Textbook of Clinical Neurology, 1st Edintrovoyz041Оценок пока нет
- Pathology of The CNS: Presented by Associated Professor/ Rehab KamalДокумент25 страницPathology of The CNS: Presented by Associated Professor/ Rehab KamalAhmed TarekОценок пока нет
- Bull 2010Документ42 страницыBull 2010László SágiОценок пока нет
- Viral Rna Universal Transport Medium Reliaprep Viral Tna KitДокумент3 страницыViral Rna Universal Transport Medium Reliaprep Viral Tna KitOLIVIA SANTAMARÍAОценок пока нет
- Blood Culture Collection and InterpretationДокумент10 страницBlood Culture Collection and InterpretationMaria Chacón CarbajalОценок пока нет
- Molecular Epidemiologic Analysis of Enterococcus FaecalisДокумент8 страницMolecular Epidemiologic Analysis of Enterococcus FaecalisoinkОценок пока нет
- Deteksi Edwardsiella Ictaluri Pada Ikan Dengan Metode Co-Agglutination TestДокумент6 страницDeteksi Edwardsiella Ictaluri Pada Ikan Dengan Metode Co-Agglutination TestN'nhieezsha Ungu CliquersОценок пока нет
- Pharmacy Council of IndiaДокумент3 страницыPharmacy Council of IndiaYuppie RajОценок пока нет
- 213 1940 1 PBДокумент5 страниц213 1940 1 PBDuma PanjaitanОценок пока нет
- 05.cultural Characheristics of BacteriaДокумент18 страниц05.cultural Characheristics of BacteriasmouteraОценок пока нет
- Microbiology and Parasitology: Exercise No. 4Документ4 страницыMicrobiology and Parasitology: Exercise No. 4Joshua James MendezОценок пока нет
- By:Ruma Daniel Hendry Kyambogo University Bsc. Human Nutrition and Dietetics. (Yr Two) TEL: 0755514951/0786224870 EmailДокумент12 страницBy:Ruma Daniel Hendry Kyambogo University Bsc. Human Nutrition and Dietetics. (Yr Two) TEL: 0755514951/0786224870 EmailRUMA DANIEL HENDRYОценок пока нет
- Annotated BibliographyДокумент6 страницAnnotated BibliographyStanley PierreОценок пока нет
- Jocel D. Oclarit-Pbs5 Finals ProjectДокумент5 страницJocel D. Oclarit-Pbs5 Finals ProjectJocel OclaritОценок пока нет
- CPH 2212 Unit 5 Written AssignmentДокумент3 страницыCPH 2212 Unit 5 Written Assignmentunclet12Оценок пока нет
- Nts Tevta Test 22-03-15 Paper BДокумент2 страницыNts Tevta Test 22-03-15 Paper BBeTechieОценок пока нет
- Wil Document Requirements Passport 1Документ3 страницыWil Document Requirements Passport 1api-283084320Оценок пока нет
- Coronavirus ReadingДокумент4 страницыCoronavirus ReadingMarianitilla MartinezОценок пока нет
- JURNAL Irma Rangkuti Dan Sisilmonalisa 1Документ14 страницJURNAL Irma Rangkuti Dan Sisilmonalisa 1Khairani PutriОценок пока нет
- Endospore Stain-WPS OfficeДокумент8 страницEndospore Stain-WPS Officejoven delos santosОценок пока нет
- Coronavirus For PDFДокумент27 страницCoronavirus For PDFlucia desantisОценок пока нет
- Anti Hiv Using Nano Robots (1) - Gajalakshmi K 20CSR049Документ10 страницAnti Hiv Using Nano Robots (1) - Gajalakshmi K 20CSR049C.V.VenkateshwaranОценок пока нет
- Isolasi Candida Albicans Dari Swab Mukosa Mulut Penderita Diabetes Melitus Tipe 2Документ7 страницIsolasi Candida Albicans Dari Swab Mukosa Mulut Penderita Diabetes Melitus Tipe 2RhmaaОценок пока нет
- CoViD19 BAGUIO CIF Ver 4 As of 9.6.2020 JAN SALENGAДокумент1 страницаCoViD19 BAGUIO CIF Ver 4 As of 9.6.2020 JAN SALENGAEjay SalengaОценок пока нет
- Encyclopedia of Virology Fourth Edition V1 5 Dennis Bamford Full ChapterДокумент67 страницEncyclopedia of Virology Fourth Edition V1 5 Dennis Bamford Full Chapterrobert.hanson139100% (5)
- MycologyyyyyyyyyyyyyyДокумент12 страницMycologyyyyyyyyyyyyyyNyxa AbdullaОценок пока нет
- 10 Diseases and Immunity IGCSE CIE Biology Ext Theory MS - UpdatedДокумент5 страниц10 Diseases and Immunity IGCSE CIE Biology Ext Theory MS - UpdatedAsma Ali KhanОценок пока нет
- DengueДокумент44 страницыDengueAl JihadОценок пока нет
- Intestinal and Luminal ProtozoaДокумент27 страницIntestinal and Luminal ProtozoatasyaghazzanniОценок пока нет