Вам также может понравиться
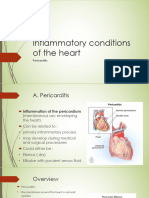
- PericarditisДокумент45 страницPericarditisBrenda WardshoneОценок пока нет
- PericarditisДокумент28 страницPericarditisHATLERОценок пока нет
- Cardiology-8 PericДокумент13 страницCardiology-8 PericMahmoud RamadanОценок пока нет
- NCM 102Документ9 страницNCM 102wooooo010056100% (1)
- PericarditisДокумент11 страницPericarditisnathan asfahaОценок пока нет
- Pericardial DiseaseДокумент11 страницPericardial Diseasenathan asfahaОценок пока нет
- Pericarditis and Pericardial EffusionДокумент31 страницаPericarditis and Pericardial EffusionDedy Chandra HariyonoОценок пока нет
- Pericarditis 65 SlidesДокумент65 страницPericarditis 65 SlidesAtifBhoreОценок пока нет
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtОт EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtРейтинг: 5 из 5 звезд5/5 (1)
- Pathophysiology of Pericardial DiseaseДокумент36 страницPathophysiology of Pericardial DiseaseivaniОценок пока нет
- Pericardial DiseseasДокумент38 страницPericardial Diseseasmameekasim75Оценок пока нет
- PericarditisДокумент52 страницыPericarditissanjivdasОценок пока нет
- Disease Rheumatic Heart DiseaseДокумент20 страницDisease Rheumatic Heart DiseaseMeena KoushalОценок пока нет
- Valvular Heart Disease: Dr. Nigussie BerihunДокумент43 страницыValvular Heart Disease: Dr. Nigussie Berihunsisay tigabuОценок пока нет
- Myocarditis and Pericarditis in ECGДокумент34 страницыMyocarditis and Pericarditis in ECGOlga GoryachevaОценок пока нет
- Diseases of The PericardiumДокумент28 страницDiseases of The PericardiumHero StoreОценок пока нет
- Examination and Investigation of The Cardiovascular System (CVS)Документ27 страницExamination and Investigation of The Cardiovascular System (CVS)Jake MillerОценок пока нет
- Angina Pectoris: Acute Coronary Syndromes (ACS)Документ18 страницAngina Pectoris: Acute Coronary Syndromes (ACS)Turky DallolОценок пока нет
- CardiovascularДокумент51 страницаCardiovascularhanthuanОценок пока нет
- Sem 11 Cardiovascular System & Dental ConsiderationsДокумент143 страницыSem 11 Cardiovascular System & Dental ConsiderationsJyoti Pol SherkhaneОценок пока нет
- Thursday Nov 3rd - BayehДокумент12 страницThursday Nov 3rd - BayehFatima MaazОценок пока нет
- Angelina A Joho MSC in Critical Care and TraumaДокумент50 страницAngelina A Joho MSC in Critical Care and TraumaZabron LuhendeОценок пока нет
- Congenital Heart Disease 1Документ14 страницCongenital Heart Disease 1OzzeyОценок пока нет
- Valvular Heart DiseaseДокумент54 страницыValvular Heart DiseaseRommanah AzmiОценок пока нет
- Cardiac Diseases During PregnancyДокумент10 страницCardiac Diseases During PregnancySandyaОценок пока нет
- Im Boards Rationalized ExamДокумент21 страницаIm Boards Rationalized Examesbat07Оценок пока нет
- PericarditisДокумент3 страницыPericarditisKhalid Mahmud Arifin0% (1)
- Media 115008 en PDFДокумент12 страницMedia 115008 en PDFsukandeОценок пока нет
- Inflammatory Disorders PDFДокумент41 страницаInflammatory Disorders PDFMoon KillerОценок пока нет
- Heart Failure: Occur TogetherДокумент5 страницHeart Failure: Occur TogetherPrince Ahmed100% (1)
- The Next Sequel: Scarring My HeartДокумент56 страницThe Next Sequel: Scarring My Heartshmily_0810Оценок пока нет
- PericarditisДокумент29 страницPericarditisPavin KumarОценок пока нет
- CVS ExaminationДокумент72 страницыCVS ExaminationPrashanthBhatОценок пока нет
- Inflamatory Heart DiseaseДокумент96 страницInflamatory Heart Diseaseأبوأحمد الحكيمОценок пока нет
- Cardiovascular System: Faisalabad Medical UniversityДокумент24 страницыCardiovascular System: Faisalabad Medical UniversityAli SohailОценок пока нет
- Cardiac Tamponade and ManagementДокумент42 страницыCardiac Tamponade and Managementأم حمدОценок пока нет
- Cardiac Tamponade (Suryani)Документ72 страницыCardiac Tamponade (Suryani)Hamdani UsmanОценок пока нет
- Congestive Heart FailureДокумент9 страницCongestive Heart FailureAbdallah Essam Al-ZireeniОценок пока нет
- Talley Sum UpДокумент51 страницаTalley Sum UpRozana Bawareth100% (1)
- Rheumatic Heart DiseaseДокумент30 страницRheumatic Heart DiseaseDhiraj PantОценок пока нет
- WK1 - Inflammatory Heart Failure Infectious DiseaseДокумент4 страницыWK1 - Inflammatory Heart Failure Infectious DiseaseJhaji Mei Margarete CasiОценок пока нет
- Cardiac Tamponade, Also Known As Pericardial Tamponade, Is AnДокумент7 страницCardiac Tamponade, Also Known As Pericardial Tamponade, Is AnSimran Josan100% (1)
- Rheumatic Heart DiseaseДокумент30 страницRheumatic Heart DiseaseshariqraipkОценок пока нет
- Assessment Cardiac SystemДокумент51 страницаAssessment Cardiac Systemejarnmd100% (2)
- Cardio FinalsДокумент18 страницCardio FinalsMoon KillerОценок пока нет
- Curs Bolile PericarduluiДокумент85 страницCurs Bolile PericarduluiAndreea ElenaОценок пока нет
- Cardiovascular System: by DR - Nuha Abdel GhaffarДокумент41 страницаCardiovascular System: by DR - Nuha Abdel GhaffarMohammed Alaa EldeanОценок пока нет
- Tiki Taka Notes Final PDFДокумент104 страницыTiki Taka Notes Final PDFAditiSahak62Оценок пока нет
- Unit 1 The History and Smmptoms Iovascular Disease: ObjectivesДокумент9 страницUnit 1 The History and Smmptoms Iovascular Disease: ObjectivesbtaleraОценок пока нет
- DR Abdulkareem Al Othman Valvular HDДокумент10 страницDR Abdulkareem Al Othman Valvular HDDarawan MirzaОценок пока нет
- LME SelfДокумент5 страницLME SelfJM Mizraime Gallo Dela-peñaОценок пока нет
- Rheumatic FeverДокумент12 страницRheumatic FeverkeikoVОценок пока нет
- 6. Митральные пороки. Клиника, диагностика, лечениеДокумент42 страницы6. Митральные пороки. Клиника, диагностика, лечениеabarna abiОценок пока нет
- Lecturio Cardiovascular Physical ExaminationДокумент10 страницLecturio Cardiovascular Physical ExaminationPranjali WeladiОценок пока нет
- Acquired Cardiac DisordersДокумент40 страницAcquired Cardiac DisordersRajaОценок пока нет
- Cardiac Tamponade: Key Points: Elevated Neck VeinsДокумент2 страницыCardiac Tamponade: Key Points: Elevated Neck VeinsPuannita SariОценок пока нет
- Pericarditis AbДокумент39 страницPericarditis AbAbnet WondimuОценок пока нет
- Pericarditis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandPericarditis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsРейтинг: 5 из 5 звезд5/5 (3)
- Pyoderma Gangrenosum Nature PrimerДокумент19 страницPyoderma Gangrenosum Nature Primerpermen_lollypopzОценок пока нет
- Rosacea, ROSCO Consensus 2019Документ8 страницRosacea, ROSCO Consensus 2019Jorge Luis Ibarra NaranjoОценок пока нет
- Sindrome Graham Little SyndromeДокумент4 страницыSindrome Graham Little SyndromeJorge Luis Ibarra NaranjoОценок пока нет
- Alfa 1 AntitripsinaДокумент9 страницAlfa 1 AntitripsinaJorge Luis Ibarra NaranjoОценок пока нет
- Tratamiento Desorden de PanicoДокумент23 страницыTratamiento Desorden de PanicoJorge Luis Ibarra NaranjoОценок пока нет
- Demencia de Cuerpos de Lewy PDFДокумент5 страницDemencia de Cuerpos de Lewy PDFÁlvaro Raúl Conto MorenoОценок пока нет
- Acute Coronary Syndrome Case-Report: A U F Angeles City College of NursingДокумент77 страницAcute Coronary Syndrome Case-Report: A U F Angeles City College of NursingCarlo Joseph Intal LlacerОценок пока нет
- Chapter 11. Cardiovascular-SystemДокумент10 страницChapter 11. Cardiovascular-SystemScianna Christel LastimosaОценок пока нет
- Pericardial Effusion With Cardiac TemponadeДокумент12 страницPericardial Effusion With Cardiac Temponademeli tswОценок пока нет
- Cardiovascular System - Printable Pages - MariebДокумент6 страницCardiovascular System - Printable Pages - MariebChristal Rae Tac-anОценок пока нет
- Visceral Manipulation in Structural Work: Liz Gaggini, M.AДокумент6 страницVisceral Manipulation in Structural Work: Liz Gaggini, M.AleoОценок пока нет
- Anatomy and Physiology WorkbookДокумент35 страницAnatomy and Physiology WorkbookMARTINОценок пока нет
- Anaphy Pre LimДокумент13 страницAnaphy Pre LimKyle M. BayangosОценок пока нет
- Ken Ham - Pocket Book - Human BodyДокумент71 страницаKen Ham - Pocket Book - Human BodyFRANKLIN CESAR GIRON RUIZОценок пока нет
- Manual Paper I FinalДокумент199 страницManual Paper I Finalankit pandey100% (1)
- Exam 1 Practice Questions Part 2Документ109 страницExam 1 Practice Questions Part 2NeoGellinОценок пока нет
- Cardiovascular SystemДокумент8 страницCardiovascular SystemDawnmurph Dharlene Wag-eОценок пока нет
- Abordaje AxilarДокумент18 страницAbordaje Axilarshoriwe68Оценок пока нет
- Bedside Emergency Cardiac Ultrasound in ChildrenДокумент11 страницBedside Emergency Cardiac Ultrasound in ChildrenNikhil KumarОценок пока нет
- Bab 20 PDFДокумент43 страницыBab 20 PDFFuad AssodiqiОценок пока нет
- Introduction in Human AnatomyДокумент60 страницIntroduction in Human AnatomyAngela Bautista85% (13)
- Module Cardiovascular System Anatomy and PhysiologyДокумент9 страницModule Cardiovascular System Anatomy and PhysiologyPATRICIA KAYE RIOОценок пока нет
- Corazon - LecturioДокумент33 страницыCorazon - LecturioFatima GiulianaОценок пока нет
- Cardiac Tamponade: Pankaj Singh Rana Nurse Practitioner in Critical Care Swami Rama Himalayan UniversityДокумент35 страницCardiac Tamponade: Pankaj Singh Rana Nurse Practitioner in Critical Care Swami Rama Himalayan UniversityBarlonga Yhan YogaОценок пока нет
- Chapter 1: Introduction To Human Anatomy and PhysiologyДокумент13 страницChapter 1: Introduction To Human Anatomy and PhysiologyElvin MoletaОценок пока нет
- Jurnal Pakai 5 (Patofisiologi, Gejala)Документ7 страницJurnal Pakai 5 (Patofisiologi, Gejala)Satrya DitaОценок пока нет
- Necropsy ManualДокумент46 страницNecropsy ManualMUSIC VIDEOSОценок пока нет
- SirkulasiДокумент17 страницSirkulasiJessica VanyaОценок пока нет
- Erwin-Sheppard Autopsy Report - Redacted by Medical ExaminerДокумент17 страницErwin-Sheppard Autopsy Report - Redacted by Medical ExaminerCheryl Sullenger100% (1)
- PHS 205 Cardiovascular SystemДокумент33 страницыPHS 205 Cardiovascular Systemdivineraymond34Оценок пока нет
- Chapter 19 Heart Marie BДокумент29 страницChapter 19 Heart Marie BomarОценок пока нет
- N3992 Practical Book of Pharmacology 2Документ12 страницN3992 Practical Book of Pharmacology 2Røxtãř RòhîťОценок пока нет
- Cardiac Tamponade: Squeezing The Heart Until It StopsДокумент4 страницыCardiac Tamponade: Squeezing The Heart Until It StopsJesse FlingОценок пока нет
- Thoracic Surgery: Cervical, Thoracic and Abdominal ApproachesДокумент1 068 страницThoracic Surgery: Cervical, Thoracic and Abdominal ApproachesAlexandru GibuОценок пока нет
- CH 13 Cardiovascular System Lecture - ACCESS - EDITSДокумент73 страницыCH 13 Cardiovascular System Lecture - ACCESS - EDITSVarel JoanОценок пока нет
- Dr. Naitik Trivedi & Dr. Upama Trivedi: Cardiovascular SystemДокумент20 страницDr. Naitik Trivedi & Dr. Upama Trivedi: Cardiovascular SystemAhmed ImranОценок пока нет