Вам также может понравиться
- Gizi Pranikah QR 2020Документ28 страницGizi Pranikah QR 2020rianОценок пока нет
- Growth Charts WHO & IAPДокумент63 страницыGrowth Charts WHO & IAPGovindan MayavanОценок пока нет
- Obesitas Pada Dewasa & Metabolisme LipidДокумент62 страницыObesitas Pada Dewasa & Metabolisme Lipidilhamaminsyaputra100% (1)
- Support Feeding - Tugas Mata Kuliah Nutrisi Klinis - Annisa FathadinaДокумент66 страницSupport Feeding - Tugas Mata Kuliah Nutrisi Klinis - Annisa FathadinaAnnisa FathadinaОценок пока нет
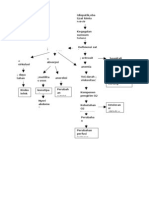
- Pathway AnemiaДокумент1 страницаPathway AnemiaRayn ChristОценок пока нет
- Visum YolaДокумент7 страницVisum YolaFarhan RahmadiОценок пока нет
- National Cholesterol Education Program: Adult Treatment Panel III (ATP III) GuidelinesДокумент103 страницыNational Cholesterol Education Program: Adult Treatment Panel III (ATP III) GuidelinesAdil AhmedОценок пока нет
- Diagnostic Approach of Short Stature / Stunted (Jan 2015) - Prof DR Jose BatubaraДокумент49 страницDiagnostic Approach of Short Stature / Stunted (Jan 2015) - Prof DR Jose BatubaraGerakan Kesehatan Ibu dan AnakОценок пока нет
- ObesityДокумент15 страницObesityKamal SaudОценок пока нет
- ID Gambaran Pemberian Asi Eksklusif Pada IbДокумент11 страницID Gambaran Pemberian Asi Eksklusif Pada IbAprilia RisqiОценок пока нет
- Samsulhadi. Dept. of Obstetric & Gynecology, Fac. of Medicine Airlangga University. Dr. Soetomo Hospital Surabaya 26 MEI 2012Документ87 страницSamsulhadi. Dept. of Obstetric & Gynecology, Fac. of Medicine Airlangga University. Dr. Soetomo Hospital Surabaya 26 MEI 2012vera anastasyaОценок пока нет
- TATA KELOLA DAN KLAIM ARSSI FEB 2022 DR HILMAN ShareДокумент40 страницTATA KELOLA DAN KLAIM ARSSI FEB 2022 DR HILMAN Sharediklat rsuannimahОценок пока нет
- Telaah Kritis JurnalДокумент13 страницTelaah Kritis JurnalfebrinaОценок пока нет
- Male InfertilityДокумент63 страницыMale InfertilitySuhaila SabanОценок пока нет
- Materi OS IDAI Aceh Dr. Dr. Anggraini Alam, Sp.A (K)Документ26 страницMateri OS IDAI Aceh Dr. Dr. Anggraini Alam, Sp.A (K)ajes coolОценок пока нет
- Ilmu Gizi Manusia Solo 2019Документ53 страницыIlmu Gizi Manusia Solo 2019Roni NurdiantoОценок пока нет
- Jadwal Pit (Fetomaternal Room)Документ3 страницыJadwal Pit (Fetomaternal Room)Dwi Adi NugrohoОценок пока нет
- Simplified weight charts for boys ages 0-12 monthsДокумент1 страницаSimplified weight charts for boys ages 0-12 monthsTheresa LauraОценок пока нет
- Anatomi Panggul, Sistem Hormonal Dan Konsepsi: Ns. Dina Mariyana.,S.KepДокумент56 страницAnatomi Panggul, Sistem Hormonal Dan Konsepsi: Ns. Dina Mariyana.,S.KepAna KareniaОценок пока нет
- Complementary Feeding or WeaningДокумент2 страницыComplementary Feeding or WeaningSumita JainОценок пока нет
- Curriculum Vitae KikiДокумент9 страницCurriculum Vitae KikiAdhe KurniawanОценок пока нет
- Post Tubal Ligation SyndromeДокумент7 страницPost Tubal Ligation SyndromeTian KapriantiОценок пока нет
- Enteral Nutrition of Preterm BabyДокумент54 страницыEnteral Nutrition of Preterm Babylordoftheweb100% (5)
- Medical Check Up: Cek KesehatanДокумент20 страницMedical Check Up: Cek KesehatanEmi PephiОценок пока нет
- STP Feeding LBW Sick NBДокумент3 страницыSTP Feeding LBW Sick NBTaran JOtОценок пока нет
- BMI-U Persentil (2-20) BoysДокумент1 страницаBMI-U Persentil (2-20) BoysHeri Hrisikesa WjgОценок пока нет
- Assisted Reproductive TechnologyДокумент41 страницаAssisted Reproductive Technologyshanty Olivia jasirwanОценок пока нет
- Diabetes in Pregnancy: DR Chippy Tess MathewДокумент29 страницDiabetes in Pregnancy: DR Chippy Tess MathewSamanmala Senarath100% (1)
- Complimentary Feeding and Problems With Complementary FeedingДокумент18 страницComplimentary Feeding and Problems With Complementary FeedinganojanОценок пока нет
- Jurnal-Intan Kemaladina (090810321)Документ10 страницJurnal-Intan Kemaladina (090810321)adindadpyanaОценок пока нет
- Ambiguous Genitalia2Документ27 страницAmbiguous Genitalia2Islam AminОценок пока нет
- Prenatal DiagnosticДокумент60 страницPrenatal DiagnosticNisaОценок пока нет
- Buku PKB 74 PDFДокумент43 страницыBuku PKB 74 PDFLissaberti AmaliahОценок пока нет
- Stunting PresentasiДокумент17 страницStunting PresentasiAxelJusuf100% (1)
- Optimizing Nutrition for Extrauterine Growth Restriction in Preterm InfantsДокумент25 страницOptimizing Nutrition for Extrauterine Growth Restriction in Preterm InfantsTitik sukamtiОценок пока нет
- Implication of Parenteral NutritionДокумент78 страницImplication of Parenteral NutritionekoОценок пока нет
- CH 5 Implantation, Placental Dev (Part1)Документ36 страницCH 5 Implantation, Placental Dev (Part1)Tengku Chairannisa PutriОценок пока нет
- Nutritional Support of Stroke Patients: ESPEN Congress Lisbon 2015Документ38 страницNutritional Support of Stroke Patients: ESPEN Congress Lisbon 2015ADIОценок пока нет
- Infant and Child Nutrition: Key PointsДокумент4 страницыInfant and Child Nutrition: Key PointsseptiОценок пока нет
- Severe Acute Malnutrition and Fluid Management inДокумент76 страницSevere Acute Malnutrition and Fluid Management inBibsОценок пока нет
- Who Reccomendation MalnutritionДокумент123 страницыWho Reccomendation MalnutritionAgaipОценок пока нет
- Keluarga Sadar Gizi (Kadarzi) Dalam Menuju Gizi Baik Untuk SemuaДокумент11 страницKeluarga Sadar Gizi (Kadarzi) Dalam Menuju Gizi Baik Untuk SemuaLutfi RensiansiОценок пока нет
- BBLRДокумент37 страницBBLRHernina OktavianiОценок пока нет
- ABORSI YANG AMAN DAN KOMPLIKASI UNSAFE ABORTIONДокумент49 страницABORSI YANG AMAN DAN KOMPLIKASI UNSAFE ABORTIONKamila Fara HanifahОценок пока нет
- CP Growth ChartДокумент30 страницCP Growth ChartJijie Azeera100% (1)
- Referat ObesitasДокумент20 страницReferat ObesitasfaisalОценок пока нет
- Centile ChartsДокумент20 страницCentile ChartsJames DaviesОценок пока нет
- Medical Nutrition Therapy For UnderweightДокумент2 страницыMedical Nutrition Therapy For UnderweightAkshaya KherОценок пока нет
- Vaginal Examinations in Labour GuidelineДокумент2 страницыVaginal Examinations in Labour GuidelinePooneethawathi Santran100% (1)
- Materi Sdidtk OkДокумент174 страницыMateri Sdidtk Okai sriyantiОценок пока нет
- ID Faktor Risiko Kejadian Stunting Pada AnaДокумент8 страницID Faktor Risiko Kejadian Stunting Pada AnaAnonymous pYR4s37H6Оценок пока нет
- CORE OBGYN 301 Syllabus 2020-2021Документ32 страницыCORE OBGYN 301 Syllabus 2020-2021smian08Оценок пока нет
- Physical and Sexual Abuse (Kuliah Power Point Blok 2)Документ39 страницPhysical and Sexual Abuse (Kuliah Power Point Blok 2)Saputra Tri Nopianto100% (1)
- ANC (Ante Natal Care) GuidelineДокумент46 страницANC (Ante Natal Care) Guidelinejason wotavizkanОценок пока нет
- Induksi Ovulasi RevДокумент38 страницInduksi Ovulasi RevBambang SulistyoОценок пока нет
- Obesitas Pada Anak: DR - Sri S.Nasar, Spa (K)Документ27 страницObesitas Pada Anak: DR - Sri S.Nasar, Spa (K)Andrie WigunaОценок пока нет
- Iron Deficiency AnemiaДокумент27 страницIron Deficiency AnemiaMargaretha MonikaОценок пока нет
- Anemia Types and TreatmentДокумент20 страницAnemia Types and TreatmentteguhxletОценок пока нет
- Nutritional Deficiencies in ChildrenДокумент69 страницNutritional Deficiencies in ChildrenRhea Mii A Cruzado75% (4)
- Pharmacy Oncology Pharmacology OutlineДокумент39 страницPharmacy Oncology Pharmacology OutlineMatthew Lei100% (1)
- Pertusis IPRM 7Документ22 страницыPertusis IPRM 7Sondang Herikson PanjaitanОценок пока нет
- Update On Child TB in IndonesiaДокумент38 страницUpdate On Child TB in IndonesiaSondang Herikson PanjaitanОценок пока нет
- Pneumonia: Unresponsive Response To Inital TreatmentДокумент25 страницPneumonia: Unresponsive Response To Inital TreatmentSondang Herikson PanjaitanОценок пока нет
- Colloid Versus Crystaloid 2012Документ44 страницыColloid Versus Crystaloid 2012Sondang Herikson PanjaitanОценок пока нет
- Resusitasi Pada AnakДокумент43 страницыResusitasi Pada AnakSondang Herikson PanjaitanОценок пока нет
- Fluid Resuscitation Guidelines for Severe Malnutrition and ObesityДокумент34 страницыFluid Resuscitation Guidelines for Severe Malnutrition and ObesitySondang Herikson PanjaitanОценок пока нет
- Pediatric Critical Care Blood Gas Analysis GuideДокумент24 страницыPediatric Critical Care Blood Gas Analysis GuideSondang Herikson PanjaitanОценок пока нет
- Transfusion-Related Acute Lung InjuryДокумент6 страницTransfusion-Related Acute Lung InjurySondang Herikson PanjaitanОценок пока нет
- PELATIHAN RESUSITASI PEDIATRIK TAHAP LANJUT SYOKДокумент28 страницPELATIHAN RESUSITASI PEDIATRIK TAHAP LANJUT SYOKSondang Herikson PanjaitanОценок пока нет
- Faktor Resiko Gagal Nafas Pada SGBДокумент5 страницFaktor Resiko Gagal Nafas Pada SGBSondang Herikson PanjaitanОценок пока нет
- Case Report Holt Oram SyndromeДокумент28 страницCase Report Holt Oram SyndromeSondang Herikson PanjaitanОценок пока нет
- Pediatric SepsisДокумент57 страницPediatric SepsisSondang Herikson PanjaitanОценок пока нет
- Developmental Milestone in ChildrenДокумент4 страницыDevelopmental Milestone in ChildrenSondang Herikson PanjaitanОценок пока нет
- Prognostic Factors and Complication Rates For Double-Filtration Plasmapheresis in Patients With Guillain-Barré SyndromeДокумент6 страницPrognostic Factors and Complication Rates For Double-Filtration Plasmapheresis in Patients With Guillain-Barré SyndromeSondang Herikson PanjaitanОценок пока нет
- SSC GuidelinesДокумент61 страницаSSC GuidelinesZfgZ*Оценок пока нет
- Complications of ApheresisДокумент7 страницComplications of ApheresisSondang Herikson PanjaitanОценок пока нет
- Pediatric Critical Care Blood Gas Analysis GuideДокумент24 страницыPediatric Critical Care Blood Gas Analysis GuideSondang Herikson PanjaitanОценок пока нет
- Manajemen of Shock in Children - Kul OnineДокумент37 страницManajemen of Shock in Children - Kul OnineSondang Herikson PanjaitanОценок пока нет
- Poster: Effect of Mendoza Protocol Therapy in Children With Steroid-Resistant Nephrotic Syndrome. A Case Series in DR - Kariadi Hospital SemarangДокумент1 страницаPoster: Effect of Mendoza Protocol Therapy in Children With Steroid-Resistant Nephrotic Syndrome. A Case Series in DR - Kariadi Hospital SemarangSondang Herikson PanjaitanОценок пока нет
- HRC Mill Approval ReportДокумент90 страницHRC Mill Approval ReportKTSivakumarОценок пока нет
- Activity Series Lab (Akey)Документ4 страницыActivity Series Lab (Akey)Elah Palaganas100% (1)
- TLV Tc1 Self Acting Temperature Regulator FlangedДокумент2 страницыTLV Tc1 Self Acting Temperature Regulator FlangedSDP02Оценок пока нет
- Equivalents of Carbon Steel QualitiesДокумент11 страницEquivalents of Carbon Steel QualitiesOscar CruzОценок пока нет
- Nutritional AnemiasДокумент33 страницыNutritional Anemiasviviyanti znОценок пока нет
- Sciencedirect: of MM CoДокумент5 страницSciencedirect: of MM CoSutan PauloОценок пока нет
- 1 Introduction of The Blast Furnace ProcessДокумент9 страниц1 Introduction of The Blast Furnace Processhemant patilОценок пока нет
- Selection of Optimum Ferronickel GradeДокумент9 страницSelection of Optimum Ferronickel GraderezaardОценок пока нет
- Basic Technology Questions Bank J.S. I 2016Документ20 страницBasic Technology Questions Bank J.S. I 2016Justus Ekene NwakaОценок пока нет
- ASME B18.8.2: Pin Materials and Hardness Pin FinishesДокумент2 страницыASME B18.8.2: Pin Materials and Hardness Pin FinishesIvan SmolejОценок пока нет
- Iron Dextran Drug StudyДокумент5 страницIron Dextran Drug StudySofronio OmboyОценок пока нет
- US3418736 Vented Steam IronДокумент3 страницыUS3418736 Vented Steam IronArturo Anaya VeraОценок пока нет
- Psychrotrophic BacteriaДокумент6 страницPsychrotrophic BacteriaMONTEALEKU100% (1)
- Identification of Cast Iron 3.1. AimДокумент8 страницIdentification of Cast Iron 3.1. AimMuruganantham anandhОценок пока нет
- Fig 1 Fe-Mn Phase DiagramДокумент3 страницыFig 1 Fe-Mn Phase DiagramAlok NayakОценок пока нет
- Types of Iron OreДокумент8 страницTypes of Iron OreParam SaxenaОценок пока нет
- Physics 10262 - Chapter 2 - Homework: Kev HG E Kev PB E Ev Z EДокумент5 страницPhysics 10262 - Chapter 2 - Homework: Kev HG E Kev PB E Ev Z ELalón Gitud De OndaОценок пока нет
- Machine Design - Selection of MaterialДокумент8 страницMachine Design - Selection of MaterialSachin Chaturvedi100% (1)
- Everything About Ductile IronДокумент5 страницEverything About Ductile IronCarlos BustamanteОценок пока нет
- HelloДокумент19 страницHelloSaroj JiОценок пока нет
- Materials Balance in Bessemer SteelmakingДокумент3 страницыMaterials Balance in Bessemer SteelmakingZarin Rafa Shaitee0% (1)
- Instant Download Essentials of Statistics 5th Edition Triola Test Bank PDF Full ChapterДокумент33 страницыInstant Download Essentials of Statistics 5th Edition Triola Test Bank PDF Full Chapterbrianhue3zqkp100% (8)
- Malleability and Metallography of Nickel - MericaДокумент28 страницMalleability and Metallography of Nickel - MericaJ. GirotoОценок пока нет
- Ferrous Sulfate (An Official Inorganic Compound) : OccurrenceДокумент11 страницFerrous Sulfate (An Official Inorganic Compound) : Occurrencehumag143Оценок пока нет
- 4 AMcKayCatalogДокумент10 страниц4 AMcKayCatalogManuelОценок пока нет
- Chemical FormulaДокумент8 страницChemical FormulaRafeeq KhanОценок пока нет
- Chanel PDFДокумент12 страницChanel PDFJefin RationalsОценок пока нет
- BF SlagДокумент9 страницBF SlagSuresh BabuОценок пока нет
- School Level Science Fair Experiments: Standard 4Документ25 страницSchool Level Science Fair Experiments: Standard 4SHAVITHA A/P MADAVAN KPM-GuruОценок пока нет
- EHB en File 9.7.3 Equivalent ASME en MaterialsДокумент3 страницыEHB en File 9.7.3 Equivalent ASME en MaterialsAdhitya DarmadiОценок пока нет