Вам также может понравиться
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Answering TechДокумент17 страницAnswering TechChiYenОценок пока нет
- Add Maths ModuleДокумент17 страницAdd Maths ModuleYap Yee SoonОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Afterschool Questions 2016 PDFДокумент144 страницыAfterschool Questions 2016 PDFKristen TeeОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Ijpp 12244Документ4 страницыIjpp 12244Kristen TeeОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Neuraminidase inhibitors block flu virus replicationДокумент1 страницаNeuraminidase inhibitors block flu virus replicationKristen TeeОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- At III TutorialДокумент20 страницAt III TutorialKristen TeeОценок пока нет
- Alien Invasion.Документ8 страницAlien Invasion.Kristen TeeОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Academic Calendar 2013-14 (Year 2)Документ1 страницаAcademic Calendar 2013-14 (Year 2)Kristen TeeОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Alien Invasion.Документ8 страницAlien Invasion.Kristen TeeОценок пока нет
- Lecture 5 HandoutДокумент7 страницLecture 5 HandoutKristen TeeОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- At III TutorialДокумент20 страницAt III TutorialKristen TeeОценок пока нет
- FadeДокумент1 страницаFadeKristen TeeОценок пока нет
- Cwu 2Документ3 страницыCwu 2Kristen TeeОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Cwu 2Документ3 страницыCwu 2Kristen TeeОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Answering TechДокумент17 страницAnswering TechChiYenОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Complications of CirrhosisДокумент2 страницыComplications of CirrhosisKristen TeeОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Development of Cinnamon Oil Based Topical Formulations for their Antibacterial ActivityДокумент17 страницDevelopment of Cinnamon Oil Based Topical Formulations for their Antibacterial ActivityKristen TeeОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
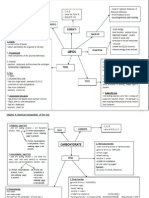
- Biology Form 4 Chapter 4 Chemical Composition Oft He CellДокумент18 страницBiology Form 4 Chapter 4 Chemical Composition Oft He CellAngie Kong Su MeiОценок пока нет
- Teaching Plan - (PHA 6663) PIP QA - 2015Документ7 страницTeaching Plan - (PHA 6663) PIP QA - 2015Kristen TeeОценок пока нет
- Tutorial With AnswerДокумент3 страницыTutorial With AnswerKristen TeeОценок пока нет
- Rabies Vaccination CertificateДокумент1 страницаRabies Vaccination CertificatevindingОценок пока нет
- HTTP: - WWW - Gurumann.com - High-BP - DIET - Ebook - by - Guru - Mann PDFДокумент8 страницHTTP: - WWW - Gurumann.com - High-BP - DIET - Ebook - by - Guru - Mann PDFVardanОценок пока нет
- Pathophysiology of Postpartum Hemorrhage and Third Stage of LaborДокумент7 страницPathophysiology of Postpartum Hemorrhage and Third Stage of Labornouval_iqbalОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Statement From Maine Veterinary Medical CenterДокумент3 страницыStatement From Maine Veterinary Medical CenterWGMEОценок пока нет
- Anatomy and Physiology of The Thyroid and Parathyroid GlandsДокумент14 страницAnatomy and Physiology of The Thyroid and Parathyroid GlandsSidiq AboobakerОценок пока нет
- Diverticular Disease 2Документ5 страницDiverticular Disease 2karl abiaadОценок пока нет
- Periodontal LigamentДокумент3 страницыPeriodontal LigamentCzarina DavidОценок пока нет
- Patriarchal Blessing Scripture FormatДокумент2 страницыPatriarchal Blessing Scripture FormatBret Richard JohnsonОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Bone Marrow Morphology: Normal and Abnormal FindingsДокумент51 страницаBone Marrow Morphology: Normal and Abnormal FindingsMohammed FareedОценок пока нет
- NCERT BookДокумент10 страницNCERT Bookkaushikray06Оценок пока нет
- Hippoboscidae Family Flies: Morphology, Life Cycle & ControlДокумент28 страницHippoboscidae Family Flies: Morphology, Life Cycle & ControlAvitus Dastan CastoОценок пока нет
- Urine Culture Test: Tests and ProceduresДокумент2 страницыUrine Culture Test: Tests and ProceduresVikashKumarОценок пока нет
- Poultry Welfare Developing CountriesДокумент12 страницPoultry Welfare Developing CountriesshamalaksОценок пока нет
- Endurence TrainingДокумент33 страницыEndurence TrainingSaxena AbhilashОценок пока нет
- 2009 Nec Hiv Dec Aidsreg2009Документ3 страницы2009 Nec Hiv Dec Aidsreg2009Jing CruzОценок пока нет
- Yoga Tips For HairLossДокумент10 страницYoga Tips For HairLossimvavОценок пока нет
- Anatomy and Physiology of the HeartДокумент56 страницAnatomy and Physiology of the Heartamjad khan100% (1)
- Scoliosis: Review of Diagnosis and Treatment: Janusz Popko, Michał Kwiatkowski, Monika GałczykДокумент5 страницScoliosis: Review of Diagnosis and Treatment: Janusz Popko, Michał Kwiatkowski, Monika Gałczykandi dirhanОценок пока нет
- Care Sheet - Axolotl (Ambystoma Mexicanum)Документ3 страницыCare Sheet - Axolotl (Ambystoma Mexicanum)John GamesbyОценок пока нет
- 1166 Stomach Dr.-RaviДокумент38 страниц1166 Stomach Dr.-RaviKubra ĖdrisОценок пока нет
- The Hall of Fire 05Документ29 страницThe Hall of Fire 05maldreidor100% (1)
- Vector - and Rodent-Borne Diseases in Europe and North America 2gfshДокумент411 страницVector - and Rodent-Borne Diseases in Europe and North America 2gfshRhyan ArfanОценок пока нет
- Marshall, 2006 Robinson, 2005 Swan and Papp, 1972: Geographic RangeДокумент24 страницыMarshall, 2006 Robinson, 2005 Swan and Papp, 1972: Geographic Rangeanggit prihatnoloОценок пока нет
- SchistosomaДокумент5 страницSchistosomasarguss14100% (1)
- Mandatory Vaccines Save Lives: Adam M. Collins ECPI University Eng120 NFHДокумент24 страницыMandatory Vaccines Save Lives: Adam M. Collins ECPI University Eng120 NFHAdam CollinsОценок пока нет
- Normal Puerperium PDFДокумент22 страницыNormal Puerperium PDFwawa3385100% (1)
- PhysiologyДокумент2 страницыPhysiologyapi-19762967Оценок пока нет
- Lessons Learned From The Dog GenomeДокумент11 страницLessons Learned From The Dog GenomebellonicoОценок пока нет
- Toshihiko Yayama - Qi Healing - The Way To A New Mind and BodyДокумент159 страницToshihiko Yayama - Qi Healing - The Way To A New Mind and BodyFernando Iglesias100% (2)
- Assisted Reproductive Technologies OverviewДокумент35 страницAssisted Reproductive Technologies OverviewPraluki HerliawanОценок пока нет