Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Diagnostics I - PulsesДокумент15 страницDiagnostics I - Pulsesg23164100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Disorders of LobesДокумент55 страницDisorders of LobesdrprasantОценок пока нет
- Clinic Theater 2 - Class 4Документ2 страницыClinic Theater 2 - Class 4drprasantОценок пока нет
- Case Study About Rectal CAДокумент11 страницCase Study About Rectal CACantiga Vhadz0% (1)
- Clinic Theater 2 - Class 5Документ2 страницыClinic Theater 2 - Class 5drprasant100% (1)
- Concepts in The Care of at Risk and Sick Adult ClientsДокумент2 страницыConcepts in The Care of at Risk and Sick Adult ClientsKiara Denise Tamayo100% (1)
- Ebook NPTE TipsДокумент11 страницEbook NPTE Tipsdrprasant100% (1)
- Blood Bank PDFДокумент178 страницBlood Bank PDFamit ingaleОценок пока нет
- Rheum MCQДокумент11 страницRheum MCQMudassar Iqbal100% (2)
- Presenting: (Diclofenac Diethylamine B.P. 100 MG)Документ2 страницыPresenting: (Diclofenac Diethylamine B.P. 100 MG)drprasantОценок пока нет
- Advised Rest and If Required Low Intensity Light Activities During The Period of T/T of 10-12 DaysДокумент2 страницыAdvised Rest and If Required Low Intensity Light Activities During The Period of T/T of 10-12 Daysdrprasant100% (1)
- Presenting: (Ketoprofen I.P. 20 MG)Документ2 страницыPresenting: (Ketoprofen I.P. 20 MG)drprasantОценок пока нет
- Given The Code in The Exhibit What Is The Result? A. B. C. D. Answer: B Explanation: ZДокумент1 страницаGiven The Code in The Exhibit What Is The Result? A. B. C. D. Answer: B Explanation: ZdrprasantОценок пока нет
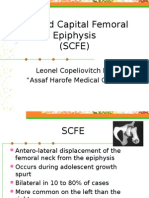
- Slipped Capital Femoral EpiphysisДокумент12 страницSlipped Capital Femoral EpiphysisdrprasantОценок пока нет
- PNF and Other TechniquesДокумент8 страницPNF and Other TechniquesdrprasantОценок пока нет
- Capri Institute of Manual Therapy: Address For Correspondence: - A-64, Hans Apartment, East Arjun Nagar, CBDДокумент1 страницаCapri Institute of Manual Therapy: Address For Correspondence: - A-64, Hans Apartment, East Arjun Nagar, CBDdrprasantОценок пока нет
- Manipulation Therapy For Tennis Elbow:-: Prasant Gupta BPT Final YearДокумент2 страницыManipulation Therapy For Tennis Elbow:-: Prasant Gupta BPT Final YeardrprasantОценок пока нет
- KiblerДокумент10 страницKiblerdrprasantОценок пока нет
- Neural Mobilizations (By David Butler) : How To Stretch A Nerve???Документ1 страницаNeural Mobilizations (By David Butler) : How To Stretch A Nerve???drprasantОценок пока нет
- 2014 Acute Hemorrhage and Blood Transfusions in Horses PDFДокумент10 страниц2014 Acute Hemorrhage and Blood Transfusions in Horses PDFCamila CalleОценок пока нет
- Mycobacterium Tuberculosis: Paper Esm MicrobiologyДокумент15 страницMycobacterium Tuberculosis: Paper Esm MicrobiologyMuhammad KurniawanОценок пока нет
- Hospital Teams: Bahasa InggrisДокумент6 страницHospital Teams: Bahasa InggrisIlhamОценок пока нет
- Impaired Verbal CommunicationДокумент6 страницImpaired Verbal CommunicationLaura Sansonetti100% (1)
- Introduction & Epidemiology Clinical Features: End-Stage Renal Disease (ESRD)Документ2 страницыIntroduction & Epidemiology Clinical Features: End-Stage Renal Disease (ESRD)Nikki VillanuevaОценок пока нет
- Parkinsons Disease FinalДокумент2 страницыParkinsons Disease Finalapi-266655633Оценок пока нет
- Late Pregnancy Bleeding (LPB) : Antepartum Hemorrhage (Aph) Dr. A. MutungiДокумент3 страницыLate Pregnancy Bleeding (LPB) : Antepartum Hemorrhage (Aph) Dr. A. Mutungikhadzx100% (2)
- Benefits of Blood DonationДокумент1 страницаBenefits of Blood DonationljxОценок пока нет
- Neck Pain ManagementДокумент35 страницNeck Pain ManagementNur Elisaa100% (1)
- Mike McKendrickДокумент61 страницаMike McKendrickVikas AgrawalОценок пока нет
- Virulence Factors of Streptococcus PyogenesДокумент6 страницVirulence Factors of Streptococcus PyogenesAmador GielasОценок пока нет
- Gynecology Adnexal MassДокумент2 страницыGynecology Adnexal MassgeОценок пока нет
- 3 ACC Prevention Blood PressureДокумент69 страниц3 ACC Prevention Blood PressureMelissa Delgado100% (1)
- List of Diseases & Afflictions: Intestinal Parasites (Stalker & Interloper)Документ2 страницыList of Diseases & Afflictions: Intestinal Parasites (Stalker & Interloper)Alex Vikingoviejo SchmidtОценок пока нет
- Gambaran Klinis Dan Patologis Pada Ayam Yang Terserang Flu Burung Sangat Patogenik (HPAI) Di Beberapa Peternakan Di Jawa Timur Dan Jawa BaratДокумент9 страницGambaran Klinis Dan Patologis Pada Ayam Yang Terserang Flu Burung Sangat Patogenik (HPAI) Di Beberapa Peternakan Di Jawa Timur Dan Jawa BaratILHAM BAGUS DARMA .NОценок пока нет
- Questions: Biographical DataДокумент7 страницQuestions: Biographical DataStephanie Claire RayaОценок пока нет
- Treatment of Hyponatremia - Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) and Reset OsmostatДокумент15 страницTreatment of Hyponatremia - Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) and Reset Osmostathoneyworks100% (1)
- IMIS BrocДокумент17 страницIMIS BrocthajeshОценок пока нет
- Hamdard Fehrist-e-Advia PDFДокумент109 страницHamdard Fehrist-e-Advia PDFdvtherion100% (1)
- Ebr - F&e OxygenationДокумент1 страницаEbr - F&e OxygenationDARLENE ROSE BONGCAWILОценок пока нет
- Cancer ReportДокумент9 страницCancer Reportcool_stud_waliОценок пока нет
- Thyroid Function Blood TestsДокумент5 страницThyroid Function Blood TestsCassandra ColigadoОценок пока нет
- JournalДокумент6 страницJournalIka RachmadantОценок пока нет
- What Are Early Indicators of Mesothelioma. Realizing The Early Signs ofДокумент2 страницыWhat Are Early Indicators of Mesothelioma. Realizing The Early Signs ofthasyaОценок пока нет
- PRECIO PromalabДокумент6 страницPRECIO PromalabJenny QuingaОценок пока нет
- I. Ecologic Model A. HypothesisДокумент5 страницI. Ecologic Model A. HypothesisTintin LevidaОценок пока нет