Вам также может понравиться
- Fat Embolism Syndrome Causes and SymptomsДокумент19 страницFat Embolism Syndrome Causes and SymptomsmuchalaithОценок пока нет
- Artritis SeptikДокумент14 страницArtritis SeptikahmadОценок пока нет
- How To Diagnose STEMI?Документ6 страницHow To Diagnose STEMI?Adhie BadriОценок пока нет
- TiroidДокумент26 страницTiroidJoni Riana MustaqimОценок пока нет
- Review Article - Mirizzi SyndromeДокумент4 страницыReview Article - Mirizzi SyndromeEvan KristionoОценок пока нет
- Kul Sem 4 Heat Stroke N Fever UHT 2016Документ63 страницыKul Sem 4 Heat Stroke N Fever UHT 2016NandaSuryaWijayaОценок пока нет
- Kuliah 16 Cor PulmonaleДокумент41 страницаKuliah 16 Cor PulmonalecaturwiraОценок пока нет
- MALARIAДокумент34 страницыMALARIALisyah FadillahОценок пока нет
- Dr. Jufri Latief (Compartment Syndromes)Документ11 страницDr. Jufri Latief (Compartment Syndromes)shintaОценок пока нет
- PRCA Causes, Symptoms, and TreatmentДокумент14 страницPRCA Causes, Symptoms, and TreatmentNikkiRoxasОценок пока нет
- HCL Update 2019 PDFДокумент8 страницHCL Update 2019 PDFHaroon KhanОценок пока нет
- Systematic Approach in Anemia Evaluation and Review of Peripheral SmearsДокумент72 страницыSystematic Approach in Anemia Evaluation and Review of Peripheral SmearsSukma Eka PratiwiОценок пока нет
- Anemi Aplastik Dan MielodisplasiaДокумент34 страницыAnemi Aplastik Dan MielodisplasiaRoby KieranОценок пока нет
- Hernia: and Other Digestive Congenital DiseaseДокумент14 страницHernia: and Other Digestive Congenital DiseaseLingga GumelarОценок пока нет
- Twin to twin transfusion syndrome الدكتور ماهر معايطةДокумент7 страницTwin to twin transfusion syndrome الدكتور ماهر معايطةjordanmedicsОценок пока нет
- Thrombosis and Embolism UPR 1Документ45 страницThrombosis and Embolism UPR 1Juan Ortega PutraОценок пока нет
- Critical Limb IschemiaДокумент11 страницCritical Limb Ischemianurliah armandОценок пока нет
- Arterial Thrombosis by AbrarДокумент20 страницArterial Thrombosis by AbrarZain HadiОценок пока нет
- Von Willebrand DiseaseДокумент14 страницVon Willebrand DiseaseCsn VittalОценок пока нет
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Документ17 страницKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaОценок пока нет
- Chronic Liver DiseaseДокумент3 страницыChronic Liver DiseaseMohammad AbbasОценок пока нет
- Disseminated Intravacular Coagulation (DIC) 2Документ12 страницDisseminated Intravacular Coagulation (DIC) 2Radya AgnaОценок пока нет
- Sindrom NefrotikДокумент22 страницыSindrom NefrotikGyta Apriati100% (1)
- Case AnakДокумент28 страницCase AnakAmorrita Puspita RatuОценок пока нет
- DEN GU E: DengueДокумент53 страницыDEN GU E: Denguerose OОценок пока нет
- Malignant Soft Tissue TumorsДокумент21 страницаMalignant Soft Tissue TumorsEva GustianiОценок пока нет
- Ricardo A. Caicedo, MD: Pediatric Gastroenterology University of FloridaДокумент20 страницRicardo A. Caicedo, MD: Pediatric Gastroenterology University of FloridaAsma SikanderОценок пока нет
- Case Report Kejang DemamДокумент48 страницCase Report Kejang DemamRahmatОценок пока нет
- Acute Pulmonary Edema - NEJMДокумент4 страницыAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- 12 - Hemostasis 1Документ21 страница12 - Hemostasis 1جووري جووري100% (1)
- Von Willebrand DiseaseДокумент14 страницVon Willebrand DiseaseJuvial DavidОценок пока нет
- PansitopeniaДокумент33 страницыPansitopeniaBrad WrightОценок пока нет
- Disseminated Intravacular Coagulation (DIC) 2Документ12 страницDisseminated Intravacular Coagulation (DIC) 2Radya AgnaОценок пока нет
- Pure Red Cell AplasiaДокумент3 страницыPure Red Cell AplasiaCitrusОценок пока нет
- Shock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentДокумент64 страницыShock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentHarika BandaruОценок пока нет
- Diagnosing and Treating Tuberculosis MeningitisДокумент6 страницDiagnosing and Treating Tuberculosis MeningitisGarrett SimpsonОценок пока нет
- Gnaps EmedicineДокумент13 страницGnaps Emedicineharyanti lupitaОценок пока нет
- Thyroid DiseasesДокумент76 страницThyroid DiseasesSolomon Fallah Foa SandyОценок пока нет
- Respiratory Diseases Commonly FoundДокумент29 страницRespiratory Diseases Commonly FoundyudhaОценок пока нет
- Timing Issues in Fracture Management: A Review of Current ConceptsДокумент9 страницTiming Issues in Fracture Management: A Review of Current ConceptsRizka Nurul FirdausОценок пока нет
- Overview of Mallory - Weiss SyndromeДокумент3 страницыOverview of Mallory - Weiss SyndromeLeslyAgredaNavarroОценок пока нет
- Management of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientДокумент12 страницManagement of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientRani Dwi NОценок пока нет
- Interna Medicine Case Report Prof. Dr. W. Z. Johannes Hospital AUGUST 2019 Medical Faculty Nusa Cendana UniversityДокумент46 страницInterna Medicine Case Report Prof. Dr. W. Z. Johannes Hospital AUGUST 2019 Medical Faculty Nusa Cendana UniversityErni JawaОценок пока нет
- MULTIPLE MYELOMA For Medical Students. Copy - 032148Документ39 страницMULTIPLE MYELOMA For Medical Students. Copy - 032148Miracle Odenigbo100% (1)
- Acs OsceДокумент4 страницыAcs OsceYohanes ArviОценок пока нет
- COVID-19 Weekly Epidemiological Update: Global OverviewДокумент31 страницаCOVID-19 Weekly Epidemiological Update: Global OverviewPaolaОценок пока нет
- PyelonephritisДокумент22 страницыPyelonephritislifespotОценок пока нет
- Management of Diabetes Mellitus in Surgical PatientsДокумент12 страницManagement of Diabetes Mellitus in Surgical PatientsAnggoro Bayu Agung DjangkaruОценок пока нет
- LEUKEMIA TYPES AND TREATMENT OPTIONSДокумент15 страницLEUKEMIA TYPES AND TREATMENT OPTIONSYon-SyuhandaОценок пока нет
- SEO-Optimized Title for PBC Case ReportДокумент40 страницSEO-Optimized Title for PBC Case Reportv_vijayakanth7656Оценок пока нет
- CV-Prof-MulyadiДокумент69 страницCV-Prof-MulyadityesОценок пока нет
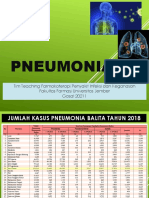
- Pneumonia: Tim Teaching Farmakoterapi Penyakit Infeksi Dan Keganasan Fakultas Farmasi Universitas Jember Gasal 20211Документ67 страницPneumonia: Tim Teaching Farmakoterapi Penyakit Infeksi Dan Keganasan Fakultas Farmasi Universitas Jember Gasal 20211Evie WulansariОценок пока нет
- Perioperative Management in Diabetes MellitusДокумент20 страницPerioperative Management in Diabetes MellitusChristopher RyalinoОценок пока нет
- AKI & Indikasi CRRTДокумент25 страницAKI & Indikasi CRRTMaya Sari BaharumОценок пока нет
- The Problem of Vascular AccessДокумент13 страницThe Problem of Vascular AccessWira DatОценок пока нет
- Comparing Antimicrobial Properties of Natural Remedies in CSFДокумент20 страницComparing Antimicrobial Properties of Natural Remedies in CSFAmalia Tri UtamiОценок пока нет
- Intrapleural Ruptured Hydatid Cyst of Liver Presented As Eosinophilic Pleural Effusion: Case ReportДокумент7 страницIntrapleural Ruptured Hydatid Cyst of Liver Presented As Eosinophilic Pleural Effusion: Case ReportIJAR JOURNALОценок пока нет
- Fat Embolism Syndrome: A Review of Pathophysiology, Diagnosis and ManagementДокумент26 страницFat Embolism Syndrome: A Review of Pathophysiology, Diagnosis and ManagementSuhanthi Mani100% (2)
- Liposuction Fat Embolism Syndrome DiagnosisДокумент5 страницLiposuction Fat Embolism Syndrome DiagnosisNgô Huỳnh ĐứcОценок пока нет
- Universidad Justo Sierra Médico Cirujano Hospital General La VillaДокумент10 страницUniversidad Justo Sierra Médico Cirujano Hospital General La VillaNancy JimenezОценок пока нет
- Shock - An OverviewДокумент19 страницShock - An OverviewHareen ReddyОценок пока нет
- Oracle QueriesДокумент15 страницOracle QueriesHareen ReddyОценок пока нет
- Non Obstetric Surgery During PregnancyДокумент64 страницыNon Obstetric Surgery During PregnancyHareen ReddyОценок пока нет
- 01 M012 36532Документ10 страниц01 M012 36532Hareen ReddyОценок пока нет
- Agile Software Development with ScrumДокумент25 страницAgile Software Development with Scrumssleandro100% (1)
- Totally Data Driven Automated TestingДокумент17 страницTotally Data Driven Automated TestingHareen ReddyОценок пока нет
- MIMS Bioterrorism 26 2015 - RAM BABUДокумент78 страницMIMS Bioterrorism 26 2015 - RAM BABUHareen ReddyОценок пока нет
- Management of Snake Bites For Alumni CME 5th Aug 2010Документ65 страницManagement of Snake Bites For Alumni CME 5th Aug 2010Hareen ReddyОценок пока нет
- Appendix DДокумент5 страницAppendix DcerisimОценок пока нет
- Testing by James BachДокумент145 страницTesting by James Bachajax248590Оценок пока нет
- Checklist For ETL Testing in Data Integration Testing ProjectДокумент1 страницаChecklist For ETL Testing in Data Integration Testing Projectwaao08100% (2)
- Totally Data Driven Automated TestingДокумент17 страницTotally Data Driven Automated TestingHareen ReddyОценок пока нет
- Hadoop TutorialДокумент62 страницыHadoop TutorialAbderrazekHmidetОценок пока нет
- AndhraYogulubook 7Документ199 страницAndhraYogulubook 7Hareen ReddyОценок пока нет
- QTP TutorialДокумент152 страницыQTP TutorialsathyakalyanОценок пока нет
- IME ClaimДокумент6 страницIME ClaimHareen ReddyОценок пока нет
- Dell - Taming The Data BeastДокумент9 страницDell - Taming The Data BeastHareen ReddyОценок пока нет
- Sample Test Plan TemplateДокумент7 страницSample Test Plan TemplateArsh WarsiОценок пока нет
- Web Site RequirementsДокумент21 страницаWeb Site RequirementsHareen ReddyОценок пока нет
- Big Data Big PotentialДокумент13 страницBig Data Big PotentialHareen ReddyОценок пока нет
- Pres 1117Документ31 страницаPres 1117Hareen ReddyОценок пока нет
- Tutorials Point, Simply Easy Learning: Java TutorialДокумент17 страницTutorials Point, Simply Easy Learning: Java TutorialAli Elsayed SalemОценок пока нет
- Cognos 8 Report Studio Lab BookДокумент94 страницыCognos 8 Report Studio Lab Booksiva_mmОценок пока нет
- Web ServicesДокумент21 страницаWeb Servicespython17Оценок пока нет
- Map ReduceДокумент28 страницMap ReduceShiva YadavОценок пока нет
- CH2 WSTechnologies V16 StandardДокумент73 страницыCH2 WSTechnologies V16 StandardHareen ReddyОценок пока нет
- Big Data Big PotentialДокумент13 страницBig Data Big PotentialHareen ReddyОценок пока нет
- Map ReduceДокумент40 страницMap ReduceHareen ReddyОценок пока нет
- ETL TestingДокумент8 страницETL TestingsurreddОценок пока нет
- Yamaha RX-A3000 - V3067Документ197 страницYamaha RX-A3000 - V3067jaysonОценок пока нет
- Biotechnology Eligibility Test (BET) For DBT-JRF Award (2010-11)Документ20 страницBiotechnology Eligibility Test (BET) For DBT-JRF Award (2010-11)Nandakumar HaorongbamОценок пока нет
- Citation GuideДокумент21 страницаCitation Guideapi-229102420Оценок пока нет
- Alpha Phi Omega National Service Fraternity Strategic PlanДокумент1 страницаAlpha Phi Omega National Service Fraternity Strategic Planlafay3tteОценок пока нет
- Lesson Plan 12 Climate ChangeДокумент5 страницLesson Plan 12 Climate ChangeRey Bello MalicayОценок пока нет
- Structural - Analysis - Skid A4401 PDFДокумент94 страницыStructural - Analysis - Skid A4401 PDFMohammed Saleem Syed Khader100% (1)
- Design Your Loyalty Program in 2 WeeksДокумент53 страницыDesign Your Loyalty Program in 2 WeeksLorena TacuryОценок пока нет
- Chapter 04Документ3 страницыChapter 04gebreОценок пока нет
- OV2640DSДокумент43 страницыOV2640DSLuis Alberto MОценок пока нет
- Basics of Duct DesignДокумент2 страницыBasics of Duct DesignRiza BahrullohОценок пока нет
- Mercury QCДокумент23 страницыMercury QCMarcus MeyerОценок пока нет
- Wei Et Al 2016Документ7 страницWei Et Al 2016Aline HunoОценок пока нет
- Case Study, g6Документ62 страницыCase Study, g6julie pearl peliyoОценок пока нет
- Ds 3805Документ4 страницыDs 3805sparky2017Оценок пока нет
- Performance of a Pelton WheelДокумент17 страницPerformance of a Pelton Wheellimakupang_matОценок пока нет
- Research of William Wells at HarvardДокумент10 страницResearch of William Wells at HarvardARGHA MANNAОценок пока нет
- Clinical Indications, Treatment and Current PracticeДокумент14 страницClinical Indications, Treatment and Current PracticefadmayulianiОценок пока нет
- Case Study - Help DocumentДокумент2 страницыCase Study - Help DocumentRahОценок пока нет
- Goes 300 S Service ManualДокумент188 страницGoes 300 S Service ManualШурик КамушкинОценок пока нет
- Guiffre V MaxwellДокумент40 страницGuiffre V MaxwellTechno Fog91% (32)
- CAM TOOL Solidworks PDFДокумент6 страницCAM TOOL Solidworks PDFHussein ZeinОценок пока нет
- Homer Christensen ResumeДокумент4 страницыHomer Christensen ResumeR. N. Homer Christensen - Inish Icaro KiОценок пока нет
- PCG Master Consultancy Services AgreementДокумент12 страницPCG Master Consultancy Services Agreementawscobie100% (1)
- Module 7 - Assessment of Learning 1 CoursepackДокумент7 страницModule 7 - Assessment of Learning 1 CoursepackZel FerrelОценок пока нет
- Earth and Beyond PDFДокумент5 страницEarth and Beyond PDFNithyananda Prabhu100% (1)
- Module-1 STSДокумент35 страницModule-1 STSMARYLIZA SAEZОценок пока нет
- Windows Keyboard Shortcuts OverviewДокумент3 страницыWindows Keyboard Shortcuts OverviewShaik Arif100% (1)
- Chapter One: Business Studies Class XI Anmol Ratna TuladharДокумент39 страницChapter One: Business Studies Class XI Anmol Ratna TuladharAahana AahanaОценок пока нет
- Unitary Small Air-Conditioners and Air-Source Heat Pumps (Includes Mixed-Match Coils) (RATED BELOW 65,000 BTU/H) Certification ProgramДокумент65 страницUnitary Small Air-Conditioners and Air-Source Heat Pumps (Includes Mixed-Match Coils) (RATED BELOW 65,000 BTU/H) Certification ProgramAmer GaladОценок пока нет
- Operating Instructions: Blu-Ray Disc™ / DVD Player BDP-S470Документ39 страницOperating Instructions: Blu-Ray Disc™ / DVD Player BDP-S470JhamОценок пока нет