Вам также может понравиться
- Pre-Op Assessment GuidelineДокумент45 страницPre-Op Assessment GuidelinearchanaОценок пока нет
- Jan LDeДокумент6 страницJan LDearchanaОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Anaesthesia Questions: Dr. Farzan Syed, Dr. Jai Prakash GuptaДокумент72 страницыAnaesthesia Questions: Dr. Farzan Syed, Dr. Jai Prakash Guptaarchana100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Pre-Op Assessment GuidelineДокумент45 страницPre-Op Assessment GuidelinearchanaОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- J R WittenbornДокумент7 страницJ R WittenbornarchanaОценок пока нет
- Turkistan IДокумент2 страницыTurkistan IarchanaОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- ASA GuidelinesДокумент34 страницыASA GuidelinesarchanaОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- NiceДокумент2 страницыNicearchanaОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
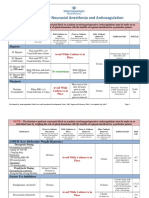
- Guidelines For Neuraxial Anesthesia and Anticoagulation: HeparinДокумент4 страницыGuidelines For Neuraxial Anesthesia and Anticoagulation: HeparinarchanaОценок пока нет
- Section of Measurement in Medicine: ModerateДокумент5 страницSection of Measurement in Medicine: ModeratearchanaОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Zeev K NДокумент6 страницZeev K NarchanaОценок пока нет
- Efficacy and Safety of Melatonin As An Anxiolytic and Analgesic in The Perioperative PeriodДокумент9 страницEfficacy and Safety of Melatonin As An Anxiolytic and Analgesic in The Perioperative PeriodarchanaОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Identifying and Assessing Anxiety in Pre-Operative PatientsДокумент1 страницаIdentifying and Assessing Anxiety in Pre-Operative PatientsarchanaОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Melatonin vs. Midazolam Premedication in Children: A Double-Blind, Placebo-Controlled StudyДокумент2 страницыMelatonin vs. Midazolam Premedication in Children: A Double-Blind, Placebo-Controlled StudyarchanaОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- M CapuzzoДокумент3 страницыM CapuzzoarchanaОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Naguib 2000Документ7 страницNaguib 2000archanaОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Naguib 2006Документ5 страницNaguib 2006archanaОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- Jan LDeДокумент6 страницJan LDearchanaОценок пока нет
- Effect of Benzodiazepine Hypnotics On All-Night Sleep EEG SpectraДокумент1 страницаEffect of Benzodiazepine Hypnotics On All-Night Sleep EEG SpectraarchanaОценок пока нет
- Premedication With Melatonin: A Double-Blind, Placebo-Controlled Comparison With MidazolamДокумент4 страницыPremedication With Melatonin: A Double-Blind, Placebo-Controlled Comparison With MidazolamarchanaОценок пока нет
- Premedication With Melatonin Vs Midazolam in Anxious ChildrenДокумент2 страницыPremedication With Melatonin Vs Midazolam in Anxious ChildrenarchanaОценок пока нет
- Effect of Benzodiazepine Hypnotics On All-Night Sleep EEG SpectraДокумент1 страницаEffect of Benzodiazepine Hypnotics On All-Night Sleep EEG SpectraarchanaОценок пока нет
- Exercize ToleranceДокумент1 страницаExercize TolerancearchanaОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Appendix 3. Pre-Operative Haemoglobin Optimisation For Elective SurgeryДокумент2 страницыAppendix 3. Pre-Operative Haemoglobin Optimisation For Elective SurgeryarchanaОценок пока нет
- Bone Cement and The Implications For AnaesthesiaДокумент6 страницBone Cement and The Implications For AnaesthesiaarchanaОценок пока нет
- Melatonin in Humans - NEJMДокумент2 страницыMelatonin in Humans - NEJMarchanaОценок пока нет
- Cardiovascular Exam GuideДокумент4 страницыCardiovascular Exam GuidearchanaОценок пока нет
- Drug AddictionДокумент8 страницDrug AddictionNgan TracKimОценок пока нет
- Australian Prescriber PDFДокумент4 страницыAustralian Prescriber PDFNadaSalsabilaОценок пока нет
- Role of Ketamine For Analgesia in Adults and ChildrenДокумент9 страницRole of Ketamine For Analgesia in Adults and ChildrenPhrily Isabell HamelbergОценок пока нет
- Acetaminophen Drug StudyДокумент2 страницыAcetaminophen Drug StudyCath Bril100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Jurnal Anestesi Bahasa InggrisДокумент15 страницJurnal Anestesi Bahasa InggrisTri Utami JasmanОценок пока нет
- Enhanced Recovery After Surgery (Eras) Protocols vs. Standard Care in Patients With Peptic Ulcer PerforationДокумент8 страницEnhanced Recovery After Surgery (Eras) Protocols vs. Standard Care in Patients With Peptic Ulcer PerforationIJAR JOURNALОценок пока нет
- Reversible Cerebral Vasoconstriction SyndromeДокумент15 страницReversible Cerebral Vasoconstriction SyndromelathifatulОценок пока нет
- Concept Map PT 1Документ1 страницаConcept Map PT 1api-657741346Оценок пока нет
- Drug Study Rle Final 1Документ18 страницDrug Study Rle Final 1YBH Construction SupplyОценок пока нет
- Feldenkrais Method Empowers Adults With Chronic.4Документ13 страницFeldenkrais Method Empowers Adults With Chronic.4Yvette M Reyes100% (1)
- Chapter 39 Pain Management in ChildrenДокумент3 страницыChapter 39 Pain Management in ChildrenAllyssa Mackinnon0% (1)
- Commentary: Novel Application For G Protein - Biased Mu Opioid Receptor Agonists in Opioid Relapse PreventionДокумент2 страницыCommentary: Novel Application For G Protein - Biased Mu Opioid Receptor Agonists in Opioid Relapse PreventionIntan AyuОценок пока нет
- Academic Sciences International Journal of Pharmacy and Pharmaceutical SciencesДокумент7 страницAcademic Sciences International Journal of Pharmacy and Pharmaceutical SciencesEdy TansilОценок пока нет
- NCP - Acute Abdominal PainДокумент3 страницыNCP - Acute Abdominal PainJet Bautista100% (2)
- Clinical Manifestations and Treatment of Osteoporotic Thoracolumbar Vertebral Compression FracturesДокумент19 страницClinical Manifestations and Treatment of Osteoporotic Thoracolumbar Vertebral Compression Fracturesmnunezh2304Оценок пока нет
- OSM Medical Mission in Baseco Provides Care for Over 1,200Документ30 страницOSM Medical Mission in Baseco Provides Care for Over 1,200Raisa Robelle Quicho69% (13)
- Leggett Announces County Suit Against 14 Opioid CompaniesДокумент163 страницыLeggett Announces County Suit Against 14 Opioid CompaniesPublic Information OfficeОценок пока нет
- A Clinical Audit Into The Success Rate of Inferior Alveolar Nerve Block Analgesia in General Dental PracticeДокумент4 страницыA Clinical Audit Into The Success Rate of Inferior Alveolar Nerve Block Analgesia in General Dental PracticeGina CastilloОценок пока нет
- Central and Peripheral Antinociceptive Activity of D. Linearis Ethanolic Leaf ExtractДокумент8 страницCentral and Peripheral Antinociceptive Activity of D. Linearis Ethanolic Leaf ExtractSdffОценок пока нет
- Emergency DrugsДокумент19 страницEmergency DrugsAdy PutroОценок пока нет
- KK Women'S & Children'S Hospital Department of Emergency Medicine Clinical GuidelinesДокумент725 страницKK Women'S & Children'S Hospital Department of Emergency Medicine Clinical GuidelinesZainal Abidin Mohd Ruslan ShahОценок пока нет
- Anatomi Dan Fisiologi NyeriДокумент183 страницыAnatomi Dan Fisiologi NyerighaliОценок пока нет
- Natural Products To Drugs Natural Product Derived CompoundsДокумент34 страницыNatural Products To Drugs Natural Product Derived CompoundsCamilo MartinezОценок пока нет
- Jaaja Bujagail Bring Back Lost Love Spell Caster +27734818506 in Tasmania Victoria West Norway Hull London MISSOURI Algeria KUWAITДокумент512 страницJaaja Bujagail Bring Back Lost Love Spell Caster +27734818506 in Tasmania Victoria West Norway Hull London MISSOURI Algeria KUWAITJohn RichОценок пока нет
- Pharmacology Lab ManualДокумент73 страницыPharmacology Lab ManualRonald Darwin58% (12)
- Pharmacology: Animation 18.1: 3D-Animation Source & Credit: Rikkyo - AcДокумент14 страницPharmacology: Animation 18.1: 3D-Animation Source & Credit: Rikkyo - AcWorld of FunОценок пока нет
- Type Drug ChartДокумент3 страницыType Drug ChartKarina Rodriguez100% (3)
- Early Management of Acute Pancreatitis-A Review of The Best Evidence. Dig Liver Dis 2017Документ32 страницыEarly Management of Acute Pancreatitis-A Review of The Best Evidence. Dig Liver Dis 2017América FloresОценок пока нет
- Clonidin Vs Tramadol For Post Spinal ShiveringДокумент4 страницыClonidin Vs Tramadol For Post Spinal ShiveringAndi Rizki CaprianusОценок пока нет
- A2 2b Rle Final DraftДокумент59 страницA2 2b Rle Final DraftQuiannë Delos ReyesОценок пока нет