Вам также может понравиться
- Guillen BarreДокумент7 страницGuillen BarreDouglas QuispeОценок пока нет
- Guillain-Barre Syndrome: Practice EssentialsДокумент16 страницGuillain-Barre Syndrome: Practice EssentialsUKMBasketОценок пока нет
- Jurnal GBSДокумент26 страницJurnal GBSfajar sugandaОценок пока нет
- Activity OverviewДокумент44 страницыActivity OverviewSnezana MihajlovicОценок пока нет
- Envejecimiento HivДокумент8 страницEnvejecimiento HivJose LunaОценок пока нет
- HealthifyPro Information CollateralДокумент11 страницHealthifyPro Information CollateralMaheshwar ReddyОценок пока нет
- Guillain-Barré SyndromeДокумент20 страницGuillain-Barré Syndromemakula densaОценок пока нет
- Bayer Annual Report 2012Документ285 страницBayer Annual Report 2012fahdlyОценок пока нет
- EMPEROR PreservedДокумент38 страницEMPEROR PreservedAppu Elias100% (1)
- Metabolic Bone DiseaseДокумент41 страницаMetabolic Bone DiseaseVenerandaОценок пока нет
- AU9560-GBS-GR: Technical Reference ManualДокумент20 страницAU9560-GBS-GR: Technical Reference ManualjobegodОценок пока нет
- Lower Motor Neuron Lesions-1Документ9 страницLower Motor Neuron Lesions-1ajay bhatОценок пока нет
- Persistent - Recurrent PneumoniaДокумент35 страницPersistent - Recurrent PneumoniaVishal SidanaОценок пока нет
- Pathological Mechanisms and Therapeutic Strategies For ADДокумент24 страницыPathological Mechanisms and Therapeutic Strategies For ADShuaib AhmadОценок пока нет
- Evaluation and Management of Young Febrile Infants 2023Документ12 страницEvaluation and Management of Young Febrile Infants 2023Felipe MayorcaОценок пока нет
- Comparative Market Analysis and Marketing Strategies 0F Videocon India LTDДокумент102 страницыComparative Market Analysis and Marketing Strategies 0F Videocon India LTDPankaj RawatОценок пока нет
- Nanoparticles For Drug Delivery: Mark BumillerДокумент32 страницыNanoparticles For Drug Delivery: Mark BumillerBogdan NeamtuОценок пока нет
- Use of Ict in Crime DetectionДокумент96 страницUse of Ict in Crime DetectionRexford AmponsahОценок пока нет
- 腰椎间盘突出症诊疗指南Документ11 страниц腰椎间盘突出症诊疗指南Fu CuОценок пока нет
- Ret B + RF: Electronic Dial Setting Thermostat With LCD Display User & Installation InstructionsДокумент97 страницRet B + RF: Electronic Dial Setting Thermostat With LCD Display User & Installation InstructionsAsmahane BenhabilesОценок пока нет
- Alogliptin - A Review of Its Use in Patients With Type 2 Diabetes MellitusДокумент20 страницAlogliptin - A Review of Its Use in Patients With Type 2 Diabetes Mellitus13201940Оценок пока нет
- Perjeta Epar Public Assessment Report - enДокумент127 страницPerjeta Epar Public Assessment Report - env9991 v9991Оценок пока нет
- Neuroanesthesiology UpdateДокумент23 страницыNeuroanesthesiology UpdateAhida VelazquezОценок пока нет
- Oxo AQAGCSE B7 ws01 XxaannДокумент2 страницыOxo AQAGCSE B7 ws01 XxaannParam BhimaniОценок пока нет
- Gullian Barre Syndrome: Department of Pharmacy Practice Kle College of Pharmacy Vidyanagar, HubballiДокумент15 страницGullian Barre Syndrome: Department of Pharmacy Practice Kle College of Pharmacy Vidyanagar, Hubballideepjyoti saikiaОценок пока нет
- Prediction of Diabetics Based On Machine LearningДокумент8 страницPrediction of Diabetics Based On Machine LearningInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- Moderated Mediation in AMOS Model 7Документ20 страницModerated Mediation in AMOS Model 7GeletaОценок пока нет
- 1 - Neuro Assessment 2021 - 336Документ30 страниц1 - Neuro Assessment 2021 - 336HADI BADWAN100% (2)
- Tubo-Ovarian Abscess - Contemporary Approach To ManagementДокумент9 страницTubo-Ovarian Abscess - Contemporary Approach To ManagementDanny. JayОценок пока нет
- ACT. A Guide To The Development of Childrens Palliative Care ServicesДокумент38 страницACT. A Guide To The Development of Childrens Palliative Care ServicesJuan Camilo SánchezОценок пока нет
- Punting and Projectile Motion Activity Worksheet TEACHER KEY - 0Документ5 страницPunting and Projectile Motion Activity Worksheet TEACHER KEY - 0Bhaskarteja PiduguОценок пока нет
- Trimble Nomad Series: ResettingДокумент3 страницыTrimble Nomad Series: ResettinglontarmyОценок пока нет
- Simple Method of EtamsylateДокумент6 страницSimple Method of EtamsylateDian NovitasariОценок пока нет
- Assessment of OrthopedicVersus Neurologic Causes of Gait Change in Dogs and CatsДокумент9 страницAssessment of OrthopedicVersus Neurologic Causes of Gait Change in Dogs and CatsAristoteles Esteban Cine VelazquezОценок пока нет
- 3122-Article Text-6458-1-10-20210709Документ23 страницы3122-Article Text-6458-1-10-20210709epiphaneОценок пока нет
- Cerebralamyloid Angiopathy: Laszlo Szidonya,, Joshua P. NickersonДокумент12 страницCerebralamyloid Angiopathy: Laszlo Szidonya,, Joshua P. NickersonJuan Carlos LazoОценок пока нет
- Insurer Market PowerДокумент7 страницInsurer Market PowerTom BiusoОценок пока нет
- CTBC Form & Consent FormДокумент2 страницыCTBC Form & Consent FormJhon Micheal AlicandoОценок пока нет
- Blockchain Based Health Monitoring and Rewarding SystemДокумент7 страницBlockchain Based Health Monitoring and Rewarding SystemInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- Neurologic Disorder FinalДокумент9 страницNeurologic Disorder FinalMary Reigns BuhatОценок пока нет
- Challan AxisДокумент3 страницыChallan AxisSumit Darak50% (2)
- 14 Principles of Management by Henri Fayol AMPAROBODOSOДокумент60 страниц14 Principles of Management by Henri Fayol AMPAROBODOSORonalyn Gaor VillegasОценок пока нет
- Mlops - Definitions, Tools and Challenges: Elated OrkДокумент8 страницMlops - Definitions, Tools and Challenges: Elated OrkNavendu BrajeshОценок пока нет
- Managerial Accounting and Cost Concepts: Curbing Administrative ExpensesДокумент33 страницыManagerial Accounting and Cost Concepts: Curbing Administrative ExpensesAdnan ButtОценок пока нет
- COVID-19 Awareness TrainingДокумент17 страницCOVID-19 Awareness TrainingAbdul Azeez OthayothОценок пока нет
- Utility of Procalcitonin in Clinical PracticeДокумент8 страницUtility of Procalcitonin in Clinical PracticeEdward ElBuenoОценок пока нет
- National Clinical GuidelinesДокумент55 страницNational Clinical GuidelinesAFH12Оценок пока нет
- Pei RanoДокумент10 страницPei RanoMayang WulanОценок пока нет
- Market and Pricing - Monopolistic Competition and OligopolyДокумент40 страницMarket and Pricing - Monopolistic Competition and OligopolyDaksh AnejaОценок пока нет
- Neonatalseizureclinicalguideline PDFДокумент15 страницNeonatalseizureclinicalguideline PDFNURUL NADIA BINTI MOHD NAZIR / UPMОценок пока нет
- What Is A Group Bible Study?Документ6 страницWhat Is A Group Bible Study?rams12380Оценок пока нет
- Sublingual Tablet Tapentadol HCL 2Документ80 страницSublingual Tablet Tapentadol HCL 2Maharshi PandyaОценок пока нет
- JURNALДокумент12 страницJURNALnuel ketarenОценок пока нет
- Schneider Preisliste 2012 NLДокумент13 страницSchneider Preisliste 2012 NLalfredopagОценок пока нет
- 020531ML Health U One Pager ICICI R1Документ1 страница020531ML Health U One Pager ICICI R1Saurabh KhareОценок пока нет
- Lesson 6 QuizДокумент3 страницыLesson 6 Quizkings zeusОценок пока нет
- Edit 430Документ101 страницаEdit 430nisp cokeovensОценок пока нет
- Lecture - Software Testing and ApplicationsДокумент30 страницLecture - Software Testing and ApplicationsKaran PatelОценок пока нет
- DR Ganesh Patil Medical StatisticsДокумент77 страницDR Ganesh Patil Medical StatisticsKaushal PatelОценок пока нет
- Guillane Barre SyndromeДокумент8 страницGuillane Barre SyndromeyasiraОценок пока нет
- Patogenesis MiopiaДокумент4 страницыPatogenesis MiopiaYolanda YaoОценок пока нет
- Patofisiologi Keracunan OrganofosfatДокумент5 страницPatofisiologi Keracunan OrganofosfatYolanda YaoОценок пока нет
- Patogenesis MiopiaДокумент4 страницыPatogenesis MiopiaYolanda YaoОценок пока нет
- Diagnosis IBSДокумент9 страницDiagnosis IBSYolanda YaoОценок пока нет
- Diferensial Diagnosa Nyeri DadaДокумент5 страницDiferensial Diagnosa Nyeri DadaYolanda YaoОценок пока нет
- Cell and DiffusionДокумент4 страницыCell and DiffusionYolanda YaoОценок пока нет
- HTML Script Tema Tumblr Blue FloralДокумент16 страницHTML Script Tema Tumblr Blue FloralYolanda YaoОценок пока нет
- PhysicsДокумент6 страницPhysicsYolanda YaoОценок пока нет
- Public Health Internship Cover LetterДокумент8 страницPublic Health Internship Cover Letterf5dct2q8100% (2)
- ERAS Protocols For Thyroid andДокумент9 страницERAS Protocols For Thyroid andOskar MartinezОценок пока нет
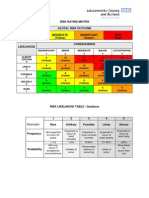
- Example of A NHS Risk Rating MatrixДокумент2 страницыExample of A NHS Risk Rating MatrixRochady SetiantoОценок пока нет
- Analytical and Hortatory ExpositionДокумент3 страницыAnalytical and Hortatory ExpositionChie TjeeОценок пока нет
- V-Gel Cleaning & User GuideДокумент3 страницыV-Gel Cleaning & User GuideInstrulife OostkampОценок пока нет
- ComplaintДокумент28 страницComplaintLia TabackmanОценок пока нет
- RLE-level-2-packet-week-12-requirement (SANAANI, NUR-FATIMA, M.)Документ26 страницRLE-level-2-packet-week-12-requirement (SANAANI, NUR-FATIMA, M.)Nur SanaaniОценок пока нет
- Pecial Eature: Transitions in Pharmacy Practice, Part 3: Effecting Change-The Three-Ring CircusДокумент7 страницPecial Eature: Transitions in Pharmacy Practice, Part 3: Effecting Change-The Three-Ring CircusSean BlackmerОценок пока нет
- Position Paper de l'UEFA Sur L'interdiction Du Gazon Synthétique Par l'ECHA 19 Juillet 2019Документ8 страницPosition Paper de l'UEFA Sur L'interdiction Du Gazon Synthétique Par l'ECHA 19 Juillet 2019LeMonde.frОценок пока нет
- 2020 HivДокумент1 страница2020 HivhenkОценок пока нет
- Test Bank For Health Psychology Biopsychosocial Interactions 9th Edition Edward P Sarafino Timothy W SmithДокумент37 страницTest Bank For Health Psychology Biopsychosocial Interactions 9th Edition Edward P Sarafino Timothy W Smithsequelundam6h17s100% (13)
- Physiological Changes Postpartum PeriodДокумент2 страницыPhysiological Changes Postpartum PeriodEurielle MioleОценок пока нет
- Understanding PTSD: Arleen Cerbone Faustina, PH.DДокумент85 страницUnderstanding PTSD: Arleen Cerbone Faustina, PH.DMuthu SelvanОценок пока нет
- Evidence-Based Practice in Pediatric Physical Therapy by BarryДокумент14 страницEvidence-Based Practice in Pediatric Physical Therapy by BarryFe TusОценок пока нет
- Types of PovertyДокумент6 страницTypes of PovertyJacobОценок пока нет
- Hirschsprung NCM 109 Case PresentationДокумент10 страницHirschsprung NCM 109 Case PresentationValerie LeddaОценок пока нет
- Group DR - Script - Allergic Rhinitis (Peanut Allergy) Health EducationДокумент10 страницGroup DR - Script - Allergic Rhinitis (Peanut Allergy) Health EducationKyra Bianca R. FamacionОценок пока нет
- Effects of Mobile Games On The Academic Performance of Grade 12 StudentsДокумент6 страницEffects of Mobile Games On The Academic Performance of Grade 12 Studentsnichole romeroОценок пока нет
- Va Tech ReportДокумент260 страницVa Tech Reportbigcee64Оценок пока нет
- The Impact of Longitudinal Studies On Understanding Development From Young Adulthood To Old AgeДокумент11 страницThe Impact of Longitudinal Studies On Understanding Development From Young Adulthood To Old AgeLana PeharОценок пока нет
- Pediatric Blood Cancer - 2022 - Mader - Social Emotional and Behavioral Functioning in Young Childhood Cancer SurvivorsДокумент11 страницPediatric Blood Cancer - 2022 - Mader - Social Emotional and Behavioral Functioning in Young Childhood Cancer SurvivorsJuliana SoaresОценок пока нет
- Helping Your Child With Extreme Picky Eating A Step-by-Step Guide For Overcoming Selective Eating, Food Aversion, and FeedingДокумент242 страницыHelping Your Child With Extreme Picky Eating A Step-by-Step Guide For Overcoming Selective Eating, Food Aversion, and FeedingAndrew Wongkar100% (3)
- Coma ManagementДокумент5 страницComa ManagementElena DocОценок пока нет
- MOHAN Di. RAJU....... MOHAN Di. RAJU......Документ32 страницыMOHAN Di. RAJU....... MOHAN Di. RAJU......Nagaraja ReddyОценок пока нет
- 2018 MUSE Inspire Conference - Show and Tell SessionsДокумент13 страниц2018 MUSE Inspire Conference - Show and Tell SessionsMichele LambertОценок пока нет
- ReferencesДокумент2 страницыReferencesapi-451063936Оценок пока нет
- IGCSE Biology (O610) Workbook: Balanced DietДокумент5 страницIGCSE Biology (O610) Workbook: Balanced DietPatrick Abidra100% (1)
- Teacher EducationДокумент32 страницыTeacher Educationsoumya satheshОценок пока нет
- Smart and Sustainable Built Environment: Article InformationДокумент14 страницSmart and Sustainable Built Environment: Article Informationmikky jayОценок пока нет
- Covid-19 and Attitudes of Ground-Level Public Health Staff in Sri LankaДокумент6 страницCovid-19 and Attitudes of Ground-Level Public Health Staff in Sri LankaIJAR JOURNALОценок пока нет