Вам также может понравиться
- Sarah Baker - The Alexander TechniqueДокумент125 страницSarah Baker - The Alexander TechniquezameershahОценок пока нет
- Flexilor RangeДокумент31 страницаFlexilor RangekurutalaОценок пока нет
- Psychopharmacologic Drugs: - Antipsychotic Agents - Antimanic Drugs - Antidepressant DrugsДокумент18 страницPsychopharmacologic Drugs: - Antipsychotic Agents - Antimanic Drugs - Antidepressant DrugsDrima EdiОценок пока нет
- Of Basques, Blood, and Blue PeopleДокумент6 страницOf Basques, Blood, and Blue PeopleVince MiglioreОценок пока нет
- Muscle RelaxantДокумент33 страницыMuscle RelaxantFady Jehad ZabenОценок пока нет
- Skeletal Muscle RelaxantsДокумент30 страницSkeletal Muscle Relaxantsmatchees-gone rogueОценок пока нет
- Onset Positions in Induction of Anesthesia Spinal Anesthesia Nitrous Oxide Respiratory Complications Respiratory ObstructionДокумент7 страницOnset Positions in Induction of Anesthesia Spinal Anesthesia Nitrous Oxide Respiratory Complications Respiratory ObstructionArvin Ian Penaflor50% (2)
- 4 Adrenergic and Anti-Adrenergic DrugsДокумент51 страница4 Adrenergic and Anti-Adrenergic DrugsLoai Mohammed IssaОценок пока нет
- Benign Prostatic Hyperplasia (BPH) : Jeselo Ouano GormeДокумент60 страницBenign Prostatic Hyperplasia (BPH) : Jeselo Ouano GormeMaddox EdeyajОценок пока нет
- Drug Study Paracetamol Ambroxol Ascorbic Acid CefuroximeДокумент5 страницDrug Study Paracetamol Ambroxol Ascorbic Acid CefuroximeCia TriiОценок пока нет
- Annex I Summary of Product CharacteristicsДокумент28 страницAnnex I Summary of Product CharacteristicsEmma SinОценок пока нет
- General AnestheticsДокумент34 страницыGeneral AnestheticsHemanathan Praem100% (1)
- Adrenoceptor Agonist and Antagonist Drugs-2014.10.7pptДокумент83 страницыAdrenoceptor Agonist and Antagonist Drugs-2014.10.7pptking_gold100% (1)
- SuxamethoniumДокумент34 страницыSuxamethoniumLee June LyngОценок пока нет
- Cholinergic Antagonists "Anticholinergic Drugs" (ParasympatholyticsДокумент32 страницыCholinergic Antagonists "Anticholinergic Drugs" (ParasympatholyticsmiznahОценок пока нет
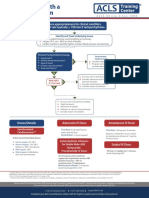
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaДокумент1 страницаAssess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaSiti Nur R Firda FauziyahОценок пока нет
- Anti-Depressant: Mohd Fikry Bin Mohamad Tahir (Student)Документ19 страницAnti-Depressant: Mohd Fikry Bin Mohamad Tahir (Student)fahmiОценок пока нет
- AnaestheticsДокумент33 страницыAnaestheticsAsif Ali LashariОценок пока нет
- Antidepressants: Depression Is One The Most Treatable Mental IllnessДокумент40 страницAntidepressants: Depression Is One The Most Treatable Mental IllnessMohammed AbdullahОценок пока нет
- Imogene KingДокумент16 страницImogene KingIsabel HernandezОценок пока нет
- Adrenergic and NonadrenergicДокумент49 страницAdrenergic and Nonadrenergicsweta sumanОценок пока нет
- Endocrine SystemДокумент21 страницаEndocrine SystemMark DimarucutОценок пока нет
- General Anesthetics AbeerДокумент45 страницGeneral Anesthetics AbeerYousef JafarОценок пока нет
- Basic Anaesthetic Drugs - SheetДокумент1 страницаBasic Anaesthetic Drugs - SheetOxigen XenonОценок пока нет
- Prefix Suffix MnemonicsДокумент5 страницPrefix Suffix MnemonicsPj MontecilloОценок пока нет
- Bioavailability and First Pass MetabolismДокумент37 страницBioavailability and First Pass MetabolismFitrye Yhana Rayyi KurniawanОценок пока нет
- Opioid Analgesics: Just in Time Training September 2006Документ16 страницOpioid Analgesics: Just in Time Training September 2006Yel CMОценок пока нет
- Printed Material Module 7 Gastrointestinal System Drugs - PDFДокумент45 страницPrinted Material Module 7 Gastrointestinal System Drugs - PDFShang MacarayonОценок пока нет
- Maternal & Child NotesДокумент19 страницMaternal & Child NotesCailah Sofia SelausoОценок пока нет
- Mayra Pagan: Pharmacology-NursingДокумент50 страницMayra Pagan: Pharmacology-NursingmayraОценок пока нет
- D. Preparing The Medication For Bolus AdministrationДокумент17 страницD. Preparing The Medication For Bolus AdministrationseanОценок пока нет
- Skeletal Muscle RelaxantsДокумент12 страницSkeletal Muscle RelaxantsKhemz Dalde LimОценок пока нет
- E.g., Phenylephrine Is Full Agonist at Alpha-Adrenoceptors. E.g., Aripipraxole Is Partial Antagonist at Selected Dopamine ReceptorsДокумент1 страницаE.g., Phenylephrine Is Full Agonist at Alpha-Adrenoceptors. E.g., Aripipraxole Is Partial Antagonist at Selected Dopamine ReceptorsSafura IjazОценок пока нет
- Drug CardsДокумент3 страницыDrug CardsDave HillОценок пока нет
- JC Stroke FinalДокумент55 страницJC Stroke FinalPleng WipolkulОценок пока нет
- CNS Stimulants PP Liley PharmДокумент30 страницCNS Stimulants PP Liley PharmJordynОценок пока нет
- A Review Sublingual Route For Systemic Drug DeliveryДокумент6 страницA Review Sublingual Route For Systemic Drug DeliveryPriambodo Gandhi100% (1)
- Different Routes of Nursing Medication AdministrationДокумент13 страницDifferent Routes of Nursing Medication AdministrationRonica MendozaОценок пока нет
- Adrenergic DrugsДокумент20 страницAdrenergic DrugsEdwardRoshanОценок пока нет
- KDT Only ClassificationsДокумент72 страницыKDT Only ClassificationsDebashis ParidaОценок пока нет
- Cholinergic and AnticholinergicДокумент77 страницCholinergic and Anticholinergicsweta sumanОценок пока нет
- OpioidsДокумент16 страницOpioidsCutie PieОценок пока нет
- Vancomycin Protocol RQHRДокумент15 страницVancomycin Protocol RQHRl1o2stОценок пока нет
- Pharmacology: Core Curriculum in NephrologyДокумент11 страницPharmacology: Core Curriculum in NephrologyYuppie RajОценок пока нет
- PancreasДокумент20 страницPancreasnarendramedaОценок пока нет
- Huntington'S Disease: Dhakal, Gerbabuena, Jittwatanatakool, Jordan, KarnДокумент25 страницHuntington'S Disease: Dhakal, Gerbabuena, Jittwatanatakool, Jordan, KarnIrene JordanОценок пока нет
- Skeletal Muscle RelaxantsДокумент11 страницSkeletal Muscle RelaxantsAhmed Al-ArwaliОценок пока нет
- Infectious DiseasesДокумент356 страницInfectious DiseasesNormala Macabuntal SaripadaОценок пока нет
- Pre AnaestheticsДокумент69 страницPre AnaestheticsPraney SlathiaОценок пока нет
- Drug Succinylcholine Atracurium Cis-Atracurium Rocuronium Vecuronium Pancuronium ED95 Intubating Dose Onset Duration MetabolismДокумент1 страницаDrug Succinylcholine Atracurium Cis-Atracurium Rocuronium Vecuronium Pancuronium ED95 Intubating Dose Onset Duration MetabolismMarshallMcGoughОценок пока нет
- Pharmacodynamic InteractionsДокумент12 страницPharmacodynamic InteractionsIshita SharmaОценок пока нет
- IV Anesthetic AgentsДокумент72 страницыIV Anesthetic AgentsRaghavendra PrasadОценок пока нет
- LocalanestheticsДокумент51 страницаLocalanestheticskingkb4uОценок пока нет
- Peak Flow MeterДокумент3 страницыPeak Flow MeterNicole PramonoОценок пока нет
- Emergency DrugsДокумент9 страницEmergency DrugsaldwinngОценок пока нет
- Intraoperative Fluid ManagementДокумент15 страницIntraoperative Fluid ManagementMirela Marina BlajОценок пока нет
- Intravenous Anesthetic Agents: by Miss Maidah MehtabДокумент49 страницIntravenous Anesthetic Agents: by Miss Maidah MehtabLuqman QadirОценок пока нет
- The Drug Act 1976Документ24 страницыThe Drug Act 1976Wàrìs Ràfìqùé ßàlòçhОценок пока нет
- Musclerelaxantandreversalagents 190313130322 PDFДокумент48 страницMusclerelaxantandreversalagents 190313130322 PDFVivek ChОценок пока нет
- Muscle RelaxantДокумент33 страницыMuscle RelaxantLivia Nathania KosasihОценок пока нет
- Muscle RelaxantДокумент35 страницMuscle RelaxantwakwawОценок пока нет
- Rheumatoid ArthritisДокумент2 страницыRheumatoid ArthritisAri Puji AstutiОценок пока нет
- Eiji Yoshikawa - Musashi 1 EarthДокумент78 страницEiji Yoshikawa - Musashi 1 EarthaerapianginОценок пока нет
- Terpenoid FriedelinДокумент4 страницыTerpenoid FriedelinAri Puji Astuti100% (1)
- A Review On Anti-Tubercular PlantsДокумент9 страницA Review On Anti-Tubercular PlantsAri Puji AstutiОценок пока нет
- Terpenoid FriedelinДокумент4 страницыTerpenoid FriedelinAri Puji Astuti100% (1)
- 060 JimenezДокумент6 страниц060 JimenezAri Puji AstutiОценок пока нет
- Anestesi Umum Dan LokalДокумент34 страницыAnestesi Umum Dan LokalAri Puji Astuti100% (1)
- Sesquiterpene Lactones - Structural Diversity and Their Biological ActivitiesДокумент22 страницыSesquiterpene Lactones - Structural Diversity and Their Biological ActivitiesAri Puji AstutiОценок пока нет
- Antiviral FarmasiДокумент46 страницAntiviral FarmasiAri Puji AstutiОценок пока нет
- Alimentary SystemДокумент47 страницAlimentary SystemAri Puji AstutiОценок пока нет
- StabiloДокумент6 страницStabiloAri Puji AstutiОценок пока нет
- Pharmacogenetics: An Introduction: Alain Li-Wan-Po and Peter Farndon Introduce The Science ofДокумент3 страницыPharmacogenetics: An Introduction: Alain Li-Wan-Po and Peter Farndon Introduce The Science ofDhuha NawabОценок пока нет
- Smejkalova - Nikola - 513281 - Bachelor ThesisДокумент86 страницSmejkalova - Nikola - 513281 - Bachelor ThesisShayn J. BenignoОценок пока нет
- The Tale of MR Jeremy FisherДокумент95 страницThe Tale of MR Jeremy FisherTrent DouglasОценок пока нет
- Toxicity of Clay Occulation of The Toxic Dino Agellate, Karenia Brevis, To Estuarine Invertebrates and SHДокумент12 страницToxicity of Clay Occulation of The Toxic Dino Agellate, Karenia Brevis, To Estuarine Invertebrates and SHinousseОценок пока нет
- Endocrine System: QuestionsДокумент15 страницEndocrine System: QuestionsJeane Irish Paller EgotОценок пока нет
- Biology Today and Tomorrow With Physiology 5th Edition Starr Solutions Manual 1Документ9 страницBiology Today and Tomorrow With Physiology 5th Edition Starr Solutions Manual 1robert100% (32)
- Chapter 18Документ31 страницаChapter 18Ali KeresteciОценок пока нет
- Corrections and Additions To Taxonomists' Glossary of Mosquito AnatomyДокумент17 страницCorrections and Additions To Taxonomists' Glossary of Mosquito AnatomymokarahОценок пока нет
- Bionic EyeДокумент1 страницаBionic EyesubhasishcОценок пока нет
- What Are The Health Benefits of Soy?Документ4 страницыWhat Are The Health Benefits of Soy?Irfan SuliansyahОценок пока нет
- Livelihood - Concepts & ApproachesДокумент19 страницLivelihood - Concepts & ApproachesMilos Nikolic100% (1)
- Review of LaboratoryДокумент48 страницReview of LaboratoryIkhar RidhoОценок пока нет
- BOS Correspondences On Chakras and AurasДокумент9 страницBOS Correspondences On Chakras and AurasDaniel EnglishОценок пока нет
- Earth and Life Science (Week 4) - q2Документ4 страницыEarth and Life Science (Week 4) - q2Rica ParillaОценок пока нет
- Unit Ii Biomedical Perspective in Gender and SexualityДокумент46 страницUnit Ii Biomedical Perspective in Gender and SexualityRowena Lanete ButaОценок пока нет
- EXERCISE 4 Stains PDFДокумент3 страницыEXERCISE 4 Stains PDFOsannah Irish InsongОценок пока нет
- General Zoology 2nd EditionДокумент274 страницыGeneral Zoology 2nd Editionhuy tanginamocccaaaaaОценок пока нет
- Unesco - Eolss Sample Chapters: History of BiologyДокумент6 страницUnesco - Eolss Sample Chapters: History of BiologyLauraLópezGiraldoОценок пока нет
- Xerophilia - V 04 No - 4-15 Dec 2015Документ110 страницXerophilia - V 04 No - 4-15 Dec 2015golf2010100% (1)
- Mammoth KillДокумент2 страницыMammoth KillLê Thị Thanh ThảoОценок пока нет
- MD FTD SARS CoV2 Assay Spec Sheet 0820 FINAL - 1800000007432513Документ2 страницыMD FTD SARS CoV2 Assay Spec Sheet 0820 FINAL - 1800000007432513tranthien.gpvОценок пока нет
- ProteinsДокумент43 страницыProteinsBilalОценок пока нет
- CV of C.v.narasimha MurthyДокумент4 страницыCV of C.v.narasimha MurthyNarasimha MurthyОценок пока нет
- Ghidul de Prevenire A Miopiei - de Dr. Kaisu VIIKARIДокумент104 страницыGhidul de Prevenire A Miopiei - de Dr. Kaisu VIIKARICristian DamocОценок пока нет
- Earth and Life Science Week 14 (Perpetuation of Life) : DECEMBER 1-4, 2020Документ9 страницEarth and Life Science Week 14 (Perpetuation of Life) : DECEMBER 1-4, 2020Ann Kyla ManrezaОценок пока нет
- Om Biomerieux Reagents Ot-43871 Package Insert-43871Документ3 страницыOm Biomerieux Reagents Ot-43871 Package Insert-43871Salomon SalomonОценок пока нет
- Dwnload Full Essentials of Understanding Psychology Canadian 5th Edition Feldman Test Bank PDFДокумент25 страницDwnload Full Essentials of Understanding Psychology Canadian 5th Edition Feldman Test Bank PDFlogosdeviatorjx3b7i100% (9)